Waseem Raja
2.2K posts

Waseem Raja
@vazim9
Interventional Cardiology Fellow @uhbtrust Birmingham,United Kingdom|MSc Clinical Trials @Oxford_NDPH|#PCI #CTO #CHIP,Structural Heart Aspirant. 🇵🇰 in 🇬🇧
Birmingham, England Katılım Eylül 2009
1.8K Takip Edilen669 Takipçiler

An honour and a privilege to attend the @SCAI Convocation Ceremony to receive the #30InTheir30s award. Congratulations to all the winners, all the FSCAI and MSCAI!
SCAI@SCAI
Congratulations to the #SCAI2026 30 in Their 30s recipients—highlighting the next generation of leaders advancing interventional cardiology through clinical excellence, research, and mentorship. 🌟👩⚕️👨⚕️ Learn more ➡️ scai.org/media-center/n… @Dr_AbuDaya @ZaidAlMarzooq @Obadah1Md @nyalborgesmd @BhattadMD @YChowdhuryMD @DocEBROhimi @fangjonathanx @HarmanSGill @KIgbalode @AhmadJabri8 @vikjag45 @ikutkutMD @NinoNJ @MukarramOsama @DrPrimeroNg @BhavanPentaMD @haseebqazi @frahman480 @sumonroy_md @drsharmatoishi @Tabaza @BWanamakerMD @ATYounesMD @JDawnAbbott1 @CCAD_MHIF @MHIF_Heart
English
Waseem Raja retweetledi

Waseem Raja retweetledi

I am not particularly surprised that the SELUTION DeNovo paper has not yet been published if this is the interpretation being promoted by the authors.
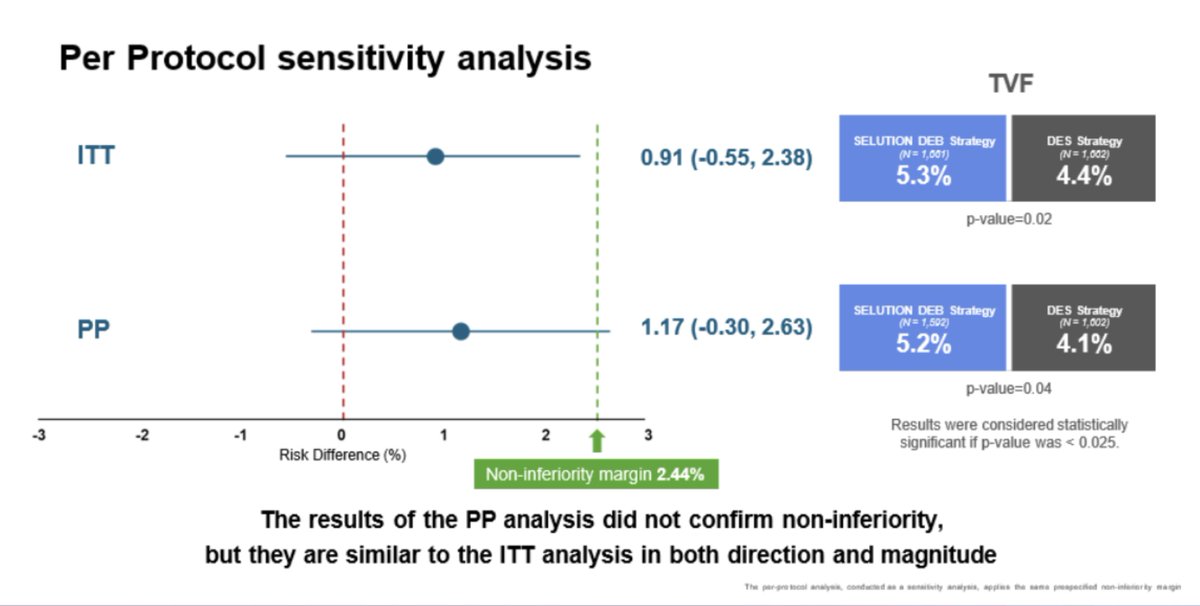
The noninferiority margin was 2.44%. In the intention-to-treat analysis, the upper bound of the risk difference for TLF was 2.38%, therefore technically meeting the criterion for noninferiority. However, in a noninferiority trial the per-protocol analysis carries greater weight, and in that analysis the upper bound of the risk difference is 2.63%, meaning that noninferiority is not achieved. To be precise, in noninferiority trials both intention-to-treat and per-protocol analyses are required, and concordant results are generally expected; when they diverge, the evidence for noninferiority is considered weak.
The authors now state that “the results of the per-protocol analysis did not confirm noninferiority, but they are similar to the intention-to-treat analysis in both direction and magnitude.” Well, where I come from we would say: “If my grandfather had wheels, he would have been a cart.”
English
Waseem Raja retweetledi

A milestone @UFHealthJax: our first tricuspid TEER, led by Dr. Ali Zgheib with Dr. Calvin Choi and imaging by Dr. Valentin Suma. Kudos to our entire heart team as we expand care for TR patients👏🫀 #TricuspidTEER #StructuralHeart #HeartTeam #Cardiology #Echo

English
Waseem Raja retweetledi


English
@cardioPCImom @CathElectroSurg Looking forward to submitting a case and attending it. Only if I could escape from cath lab!
English

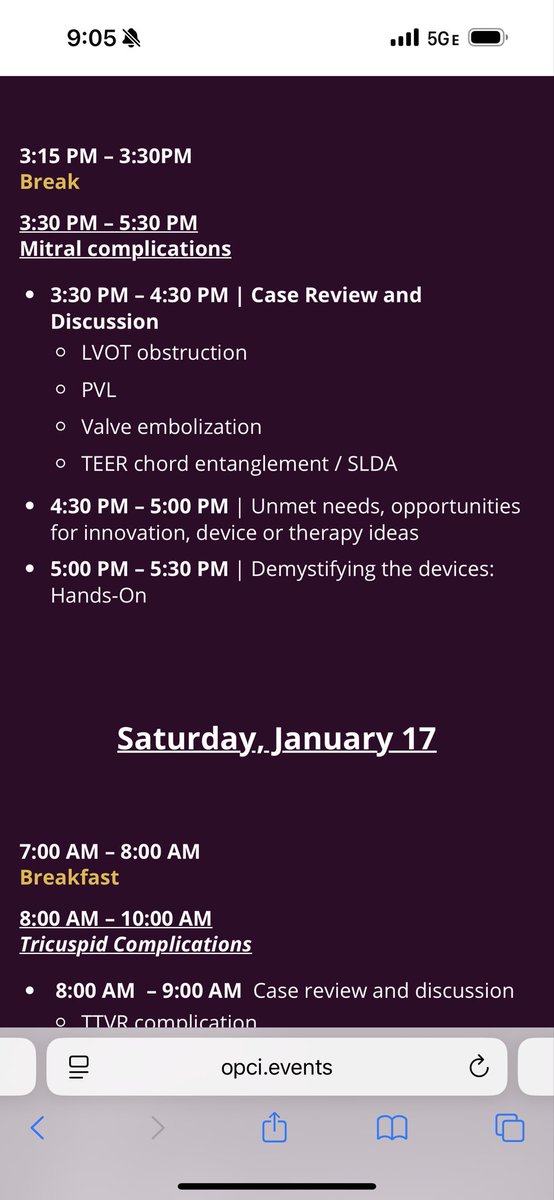
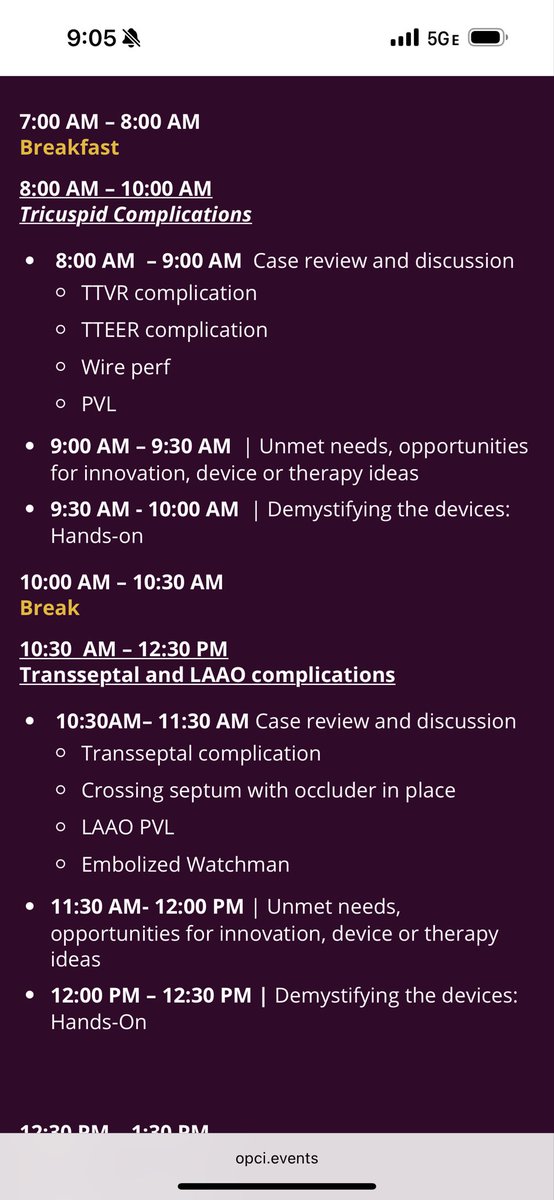
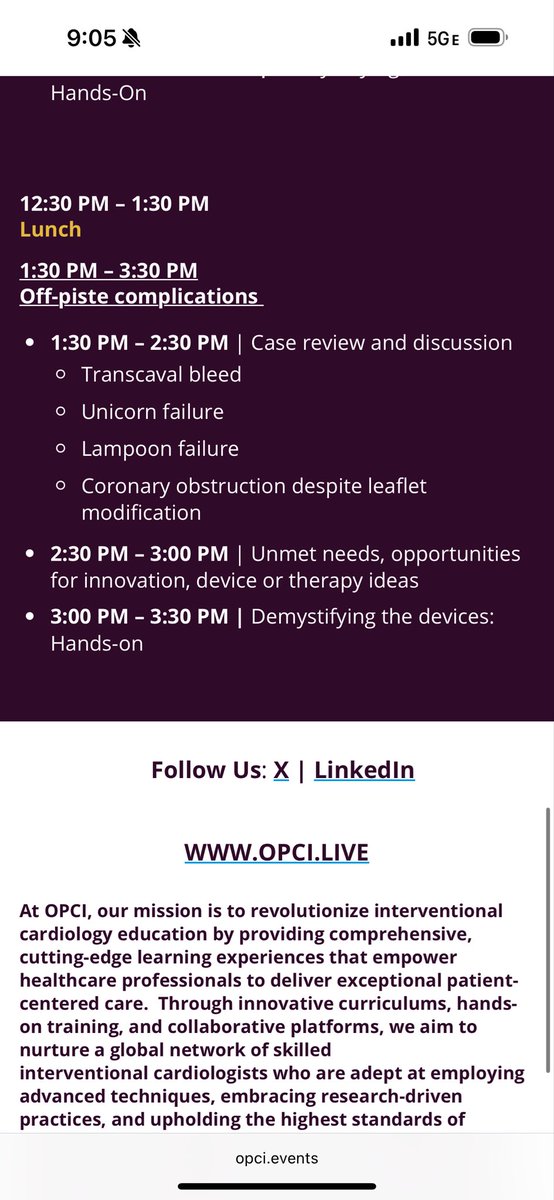
Incredibly excited to attend this course! Agenda now posted - hope many others join! @CathElectroSurg

OPCI@OPCILive
OPCI Structural Complications Summit 2026 | Salt Lake City, January 16 -17 📅 Register at opci.events/event/structur… CALL FOR CASES! Fellows: Submit a case upon registration. If selected, OPCI will cover airfare and 2-night stay. ✈️🏨 Stay and ski MLK weekend ⛷️🏔️ Build best practices on how to avoid and manage complications as well as explore opportunities for innovation. Sessions will discuss strategies for coping with the emotional impact these situations can have on operator and teams. #cardiotwitter @CathElectroSurg
English
Waseem Raja retweetledi

#CVRjax Thanks to Prof. @CMichaelGibson for discussing the findings of this interesting study assessing the impact of race on platelet reactivity and clinical outcomes after PCI.
C. Michael Gibson MD@CMichaelGibson
Dr. Ortega and Dr. Gibson discuss the intersection of race and platelet function, as well as the disparities in clinical outcomes among different racial groups. @Ortega_Paz @UFHealthJax
English
@Ortega_Paz @CMichaelGibson @UFHealthJax @mirvatalasnag @sbrugaletta @Hragy @EricTopol @DrPascalMeier @DrMarthaGulati @drjohnm @HeartOTXHeartMD @HeartBobH @DrSethdb @hmkyale @DrSheilaSahni @DLBHATTMD @gina_lundberg @MWaltonShirley @ErinMichos @AjayKirtane @GreggWStone @rwyeh @SVRaoMD @DrToniyaSingh @DocSavageTJU @keaglemd @MinnowWalsh @DrKevinCampbell @HeartDocSharon @DrDave01 @josejgdnews @JonHsuMD @MKIttlesonMD @LisaRosenbaum17 @mmamas1973 @ziadalinyc @sahilparikhmd @JavedButler1 @kaulcsmc @HighSTEACS @HeartDocSadiya @kovacic_jason @RonBlankstein @KaulP @sjauhar @AmitGoyalMD @EdwardFryMD @TCTMD_Yael @TCTMD @PCRonline Very informative study and even better presentation. Thanks for sharing.
English
@CMichaelGibson @UFHealthJax @mirvatalasnag @sbrugaletta @Hragy @EricTopol @DrPascalMeier @DrMarthaGulati @drjohnm @HeartOTXHeartMD @HeartBobH @DrSethdb @hmkyale @DrSheilaSahni @DLBHATTMD @gina_lundberg @MWaltonShirley @ErinMichos @AjayKirtane @GreggWStone @rwyeh @SVRaoMD @DrToniyaSingh @DocSavageTJU @keaglemd @MinnowWalsh @DrKevinCampbell @HeartDocSharon @DrDave01 @josejgdnews @JonHsuMD @MKIttlesonMD @LisaRosenbaum17 @mmamas1973 @ziadalinyc @sahilparikhmd
@JavedButler1 @kaulcsmc @HighSTEACS
@HeartDocSadiya @kovacic_jason @RonBlankstein
@KaulP @sjauhar @AmitGoyalMD @EdwardFryMD @TCTMD_Yael @TCTMD @PCRonline @ESC_Journals
QAM
Dr. Ortega and Dr. Gibson discuss the intersection of race and platelet function, as well as the disparities in clinical outcomes among different racial groups. @Ortega_Paz @UFHealthJax
English
SELUTION DeNovo met its primary endpoint of noninferiority at 1 year, with “only” 20% of DES required as bailout in the drug-coated balloon arm. Imaging use was limited in both groups, while specialty balloons were more frequently employed in the DCB+DES arm (though not dramatically so)—a consequence of randomization occurring before predilatation. There was applause in the room, but the full publication is still pending, so caution is warranted. This is particularly true since analyses were reported as intention-to-treat, which in a noninferiority trial does not tell the whole story (it would be important to see the as-treated and per-protocol analyses), and because some statistical interactions were not immediately clear and somewhat counterintuitive. In any case, an absolute difference of 0.9% between the two arms appears acceptable at 1 year, especially if noninferiority is maintained at 5 years and a benefit emerges consistent with the expected advantages of leave-nothing-behind strategies. #TCT2025
Davide Capodanno@DFCapodanno
The most anticipated trial at next #TCT2025 is SELUTION DeNovo. So let’s take a closer look. This study represents an important crossroads for drug-coated balloons (DCBs) in de novo lesions, since—apart from small vessels—the results so far have been far from impressive. Let’s start with the study population, which includes patients with at least one vessel to be treated, ranging from 2 to 5 mm in diameter. This means that some vessels would typically be treated with a DCB, while others would more commonly receive a drug-eluting stent (DES). Naturally, a proportion of patients initially intended for DCB treatment will end up with a stent—for example, in the case of a dissection or when, after predilatation, the operator feels uncomfortable leaving the vessel without one. This should not be interpreted as a crossover, but rather as part of the treatment strategy being tested. In fact, randomization occurs before predilatation, unlike in other studies. Investigators expect this to happen in no more than 30% of cases—which is not negligible. In other words, the trial aims to avoid stenting and pursue a “leave nothing behind” approach in about 70% of cases. Then there is the DCB itself, which is coated with sirolimus. In theory, sirolimus is not the perfect drug for this use, given its low lipophilicity. However, it has other advantages—lower cytotoxicity and stronger inhibition of neointimal proliferation. In this specific balloon, the microreservoir design is meant to retain the drug, preventing distal embolization and ensuring homogeneous drug delivery for up to 90 days. This means that negative results from previous DCB trials should not automatically be generalized to all DCBs—though this, of course, remains to be seen. Finally, the study hypothesis: noninferiority at 1 and 5 years (with 1-year results expected at TCT). If noninferiority is demonstrated, superiority will also be tested. Investigators expect a 6% event rate in both arms at 1 year and have set a noninferiority margin of 3%. Should the observed event rate be lower than expected—which, as we know, often happens in this type of trial—the margin will be tightened to 2.5%, with statistical power reduced from 95% to 90%. A smart and pragmatic choice. Moreover, the sample size is substantial: 3,326 patients, making this the largest trial ever conducted in this field. Since current guidelines recommend DCBs only for in-stent restenosis, SELUTION DeNovo has the potential to expand indications to de novo coronary lesions—potentially shifting part of the field from drug-eluting stents to drug-coated balloons, if the trial results are positive. It’s an evolving landscape, with emerging contenders such as bioadaptors and, inevitably, a comeback of bioresorbable scaffolds sooner or later.
English
@kaulcsmc @DFCapodanno Though it’s a strategy trial, but how 20% SEB arm getting a stent becomes strength of this trial design. Though event rate was 5% in those “80%” who only received SEB.
English

@DFCapodanno 1/
Unusual choice of margin: 50% of TVF rates of SEB plus DES combined [(4.4+5.3)/2]*0.5 = 2.44%
RR margin =(4.4%+2.44%)/4.4% = 1.55
To accept up to 55% inferiority of SEB, it should offer some advantages in safety (bleeding), cost or convenience.
English

@DFCapodanno Great summary. Looking forward to the results. If it will be ITT analysis, and 30% end up having DES after pre-dilatation, won’t it affect study power?
English
The most anticipated trial at next #TCT2025 is SELUTION DeNovo. So let’s take a closer look. This study represents an important crossroads for drug-coated balloons (DCBs) in de novo lesions, since—apart from small vessels—the results so far have been far from impressive.
Let’s start with the study population, which includes patients with at least one vessel to be treated, ranging from 2 to 5 mm in diameter. This means that some vessels would typically be treated with a DCB, while others would more commonly receive a drug-eluting stent (DES). Naturally, a proportion of patients initially intended for DCB treatment will end up with a stent—for example, in the case of a dissection or when, after predilatation, the operator feels uncomfortable leaving the vessel without one. This should not be interpreted as a crossover, but rather as part of the treatment strategy being tested. In fact, randomization occurs before predilatation, unlike in other studies. Investigators expect this to happen in no more than 30% of cases—which is not negligible. In other words, the trial aims to avoid stenting and pursue a “leave nothing behind” approach in about 70% of cases.
Then there is the DCB itself, which is coated with sirolimus. In theory, sirolimus is not the perfect drug for this use, given its low lipophilicity. However, it has other advantages—lower cytotoxicity and stronger inhibition of neointimal proliferation. In this specific balloon, the microreservoir design is meant to retain the drug, preventing distal embolization and ensuring homogeneous drug delivery for up to 90 days. This means that negative results from previous DCB trials should not automatically be generalized to all DCBs—though this, of course, remains to be seen.
Finally, the study hypothesis: noninferiority at 1 and 5 years (with 1-year results expected at TCT). If noninferiority is demonstrated, superiority will also be tested. Investigators expect a 6% event rate in both arms at 1 year and have set a noninferiority margin of 3%. Should the observed event rate be lower than expected—which, as we know, often happens in this type of trial—the margin will be tightened to 2.5%, with statistical power reduced from 95% to 90%. A smart and pragmatic choice. Moreover, the sample size is substantial: 3,326 patients, making this the largest trial ever conducted in this field.
Since current guidelines recommend DCBs only for in-stent restenosis, SELUTION DeNovo has the potential to expand indications to de novo coronary lesions—potentially shifting part of the field from drug-eluting stents to drug-coated balloons, if the trial results are positive. It’s an evolving landscape, with emerging contenders such as bioadaptors and, inevitably, a comeback of bioresorbable scaffolds sooner or later.

English
Waseem Raja retweetledi
JACC Journals@JACCJournals
Fibrinolytic therapy remains a major mgmt option for thromboembolic diseases. Advances in catheter-directed techniques, dosing strategies, & novel agents may expand therapeutic options & improve the safety of fibrinolytic therapy. jacc.org/doi/10.1016/j.… #JACC @bbikdeli @hmkyale
QHT

Pakistan will face New Zealand or Korea in the final at 6:00pm (PST) tomorrow. Mark your calendars! 🇵🇰🏑
#FIHNationsCup

English
@BaoGTran I will be keen to avoid another bifurcation for this PCI- pending IVUS. Another stent to LAD after bifurcation and DCB to other branches with final KBI with DCB in LAD-D1.

English

What is your PCI strategy?
Old stents in only proximal part of LAD and also in diag.
On IVUS LAD is 4.5mm proximal and 3mm distal to bifurcation
English

This guy is crazy.
Cinema Tweets@CinemaTweets1
FIRST LOOK: Christian Bale as Al Davis in the Upcoming Film “Madden”
English
@LAzzaliniMD I believe it’s always the first spurt of contrast on a step by step advancement of frames. Building on the same, I can see ping-pong catheter. Depending on the guide catheter chosen what’s your experience with “block and deliver technique”.
English


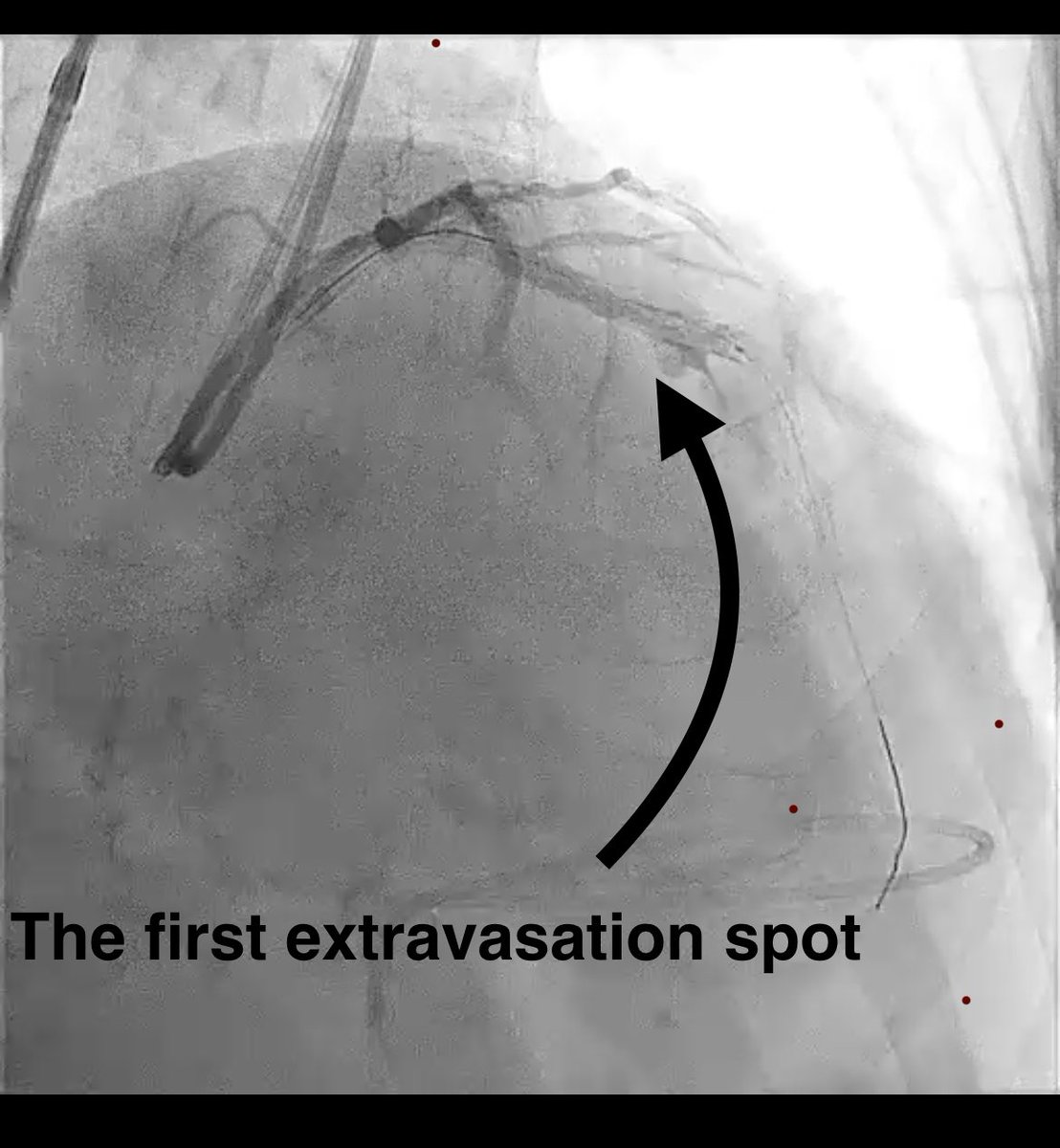
A perforation developed after stenting.
Where is the perforation?
(see video and picture in the thread)
English

I am graduating from a prestigious interventional program at Massachusetts General Hospital this month!
I am very honored to be a part of the cath lab at MGH and I really appreciate all the support from the program/faculty and staff!

English
just clocked we are already half way through 2025.
Hahahahahahahaha
English