Sabitlenmiş Tweet

Mutations are expected in genome. Now we already have a mutation in SARS-CoV2, are there (machine learning) algorithms efficient enough to predict mutations in sars cov2?
English
Vishal Parekh
766 posts

@vishalsp10
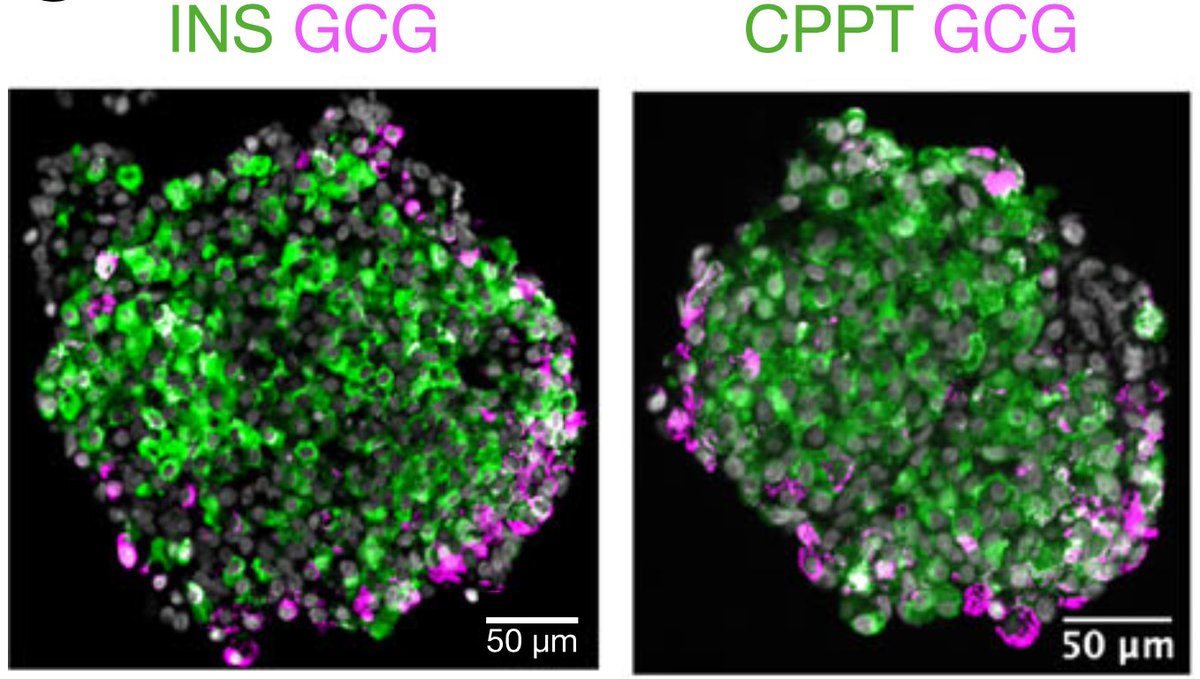
🇮🇳🇸🇪 a proud father was @DBT_NCCS_Pune, @UmeaFor, @UMPharmacology, & @Broadinstitute Islet cells| Diabetes|




Great to meet Stephen Coombes & Kyle Wedgwood at this year’s #BMCBAMC2025 in Exeter! Their new book Neurodynamics: An Applied Mathematics Perspective (Springer TAM series) is a fantastic deep dive into the math of brain dynamics. 📘🧠 Highly recommended! #AppliedMath






𝐈𝐦𝐦𝐮𝐧𝐨𝐠𝐞𝐧𝐢𝐜𝐢𝐭𝐲 is the ability of a substance such as an antigen or epitope to trigger an immune response in the host. To learn more about this NEJM Illustrated Glossary term, read the Clinical Implications of Basic Research article “Novel Proteins to Neutralize Venom Toxins” from @UniversidadCR: nej.md/4kKngiv Explore more terms: nej.md/glossary