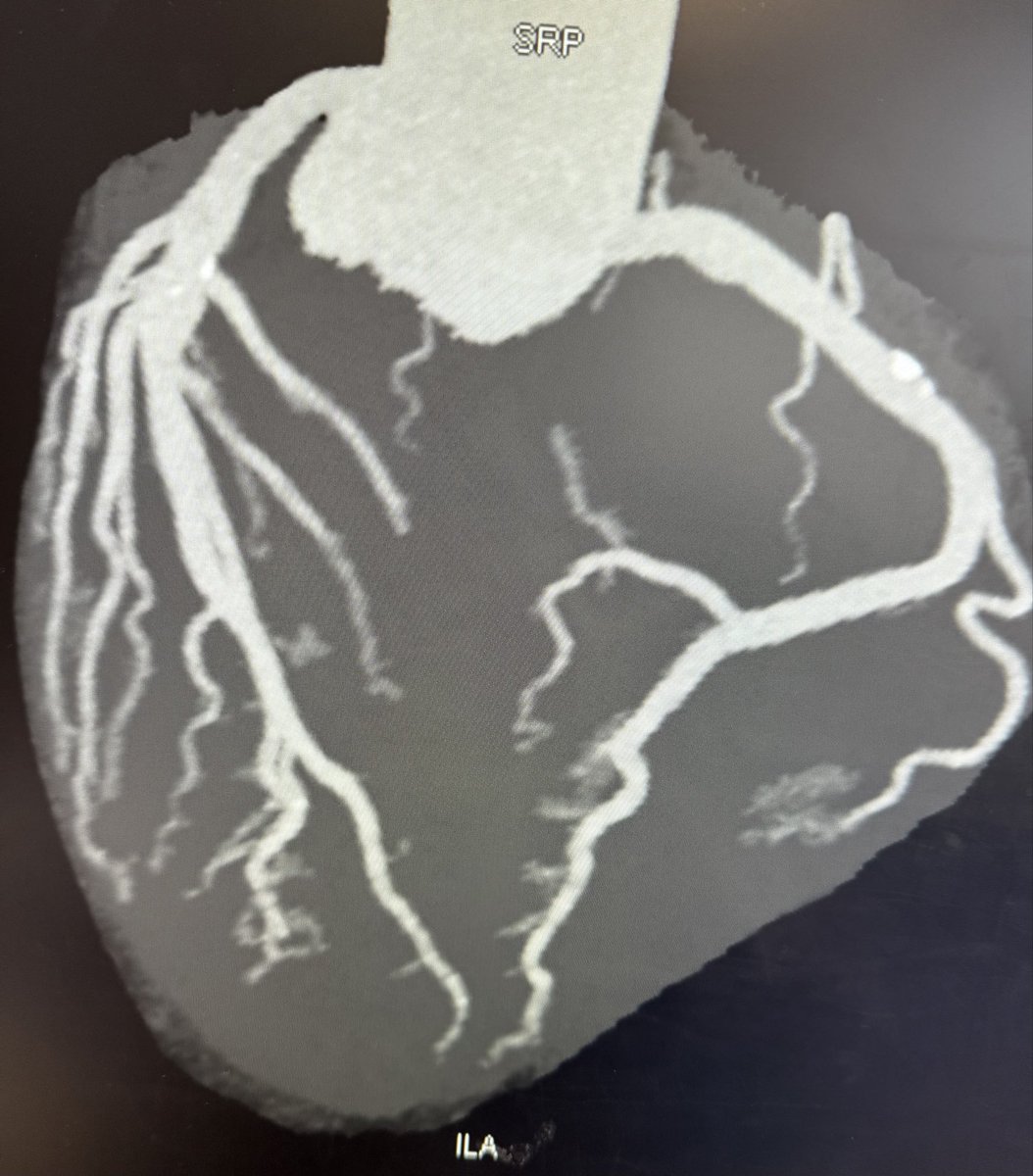
@misamed @SOCiME_ @solaci_online @smexcardiologia @AncisssteMx Look like thick part of septum ? Is it really true FO in angio ?
English
okap
2.5K posts
@hellojoni
born in fabric , grow up in the kitchen


Panie Pawle, brakuje Panu jak to często z Panem bywa obiektywizmu. W Polsce takie badania proponuje się między 50 a 65 rokiem życie. Dla zdrowej osoby w wieku objętym polskim programem przesiewowym bez poważnych chorób współistniejących prawdopodobieństwo, że rozwinie się u niej rak jelita grubego, który nigdy nie zostanie wykryty i nigdy nie doprowadzi do jej śmierci, jest bardzo niskie. Szacunkowo 0,2 do 0,4 % w ciągu całego życia a nawet niżej. Oczywiście w tym wieku już nie wszyscy są zdrowi. Więc ogólnie tym badaniu w tej grupie wiekowej 2-4% wykrytych raków j. grubego nie zdążyłoby zagrozić życiu bo osoba, która by miała raka zdąży umrzeć z jakiegoś innego powodu. Ludzie to generalnie rozumieją. Ale pan profilaktykę jak zwykle demonizuje.


PILNE. Jest wyrok w sprawie #Pfizer-Polska. Będziemy musieli zapłacić 5,6 mld zł za nieodebrane szczepionki przeciw Covid-19


@marek_2k22 Mnie to, że oddają nie przeraża ale to ILE tego ludzie oddają, ja to zgrzewke wody na tydzień z partnerką wypije a tam ludzie co chwilę z pełnymi torbami przychodzą

Clopidogrel is superior to aspirin for cardiac outcomes beyond 1-year up to 5-years. Results from the STOPDAPT-2 ACS and STOPDAPT-2 Total Cohort. Should it be a lifelong maintenance therapy? @HirotWatanabeMD @MNatsuaki @KoYamamoto7 ahajrnls.org/3PlxLhD

Zaczynam dyżur na psychiatrii, kolejny dyżur w niedzielę, a z wolnymi miejscami na oddziale bardzo licho. Będzie ciekawy weekend...


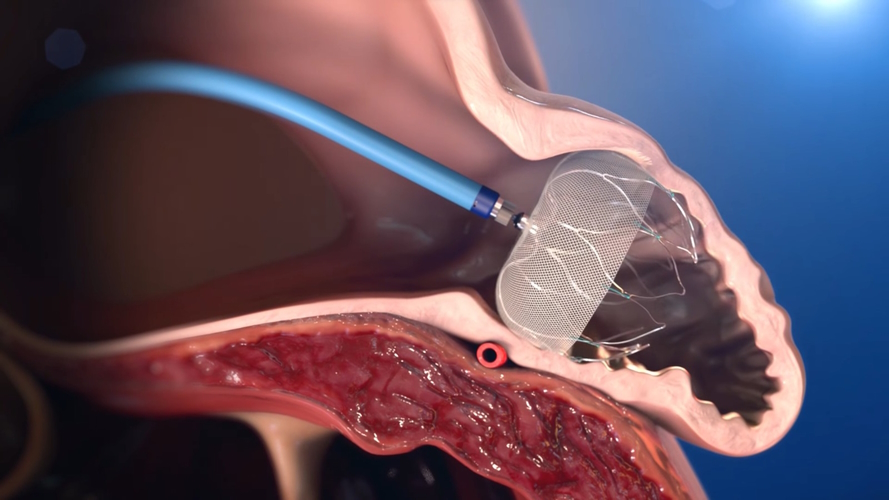



Among patients with atrial fibrillation at high risk for stroke and bleeding, left atrial appendage closure was not noninferior to medical therapy in reducing the risk of stroke, embolism, major bleeding, or death at 3 years. Full CLOSURE-AF trial results: nejm.org/doi/full/10.10… Editorial: Left Atrial Appendage Closure — Another Overused Method in Cardiology? nejm.org/doi/full/10.10…
@djc795 @drjohnm Major bleeding (-1.2/100 PY) and CV death/unexplained death (-1.8/100 PY) drove the PEP in favor of best medical care. There was no good reason to chose LAAC over OAC. It was made up to justify approval without any RCT evidence to back it up.