@SPuro88 @AshleyGWinter Esp when it’s 25 miles from the hospital I’m rounding at….
English
Jonathan Pavlinec, MD
2K posts

@jpavs17
Fellowship trained Endourology & Robotic Surgeon Prostate Cancer/BPH/Stones focus, Triple🐊, and native Floridian


North Carolina Hospitals have deployed these telepresence robots These allow doctors to interact remotely with patients. A real human doctor is operating this remotely and speaking with patients Yes, this is real. This is so dystopian North Carolina hospitals deployed these to combat doctor burnout and staffing shortages at some locations
I'm 36. I'm a physician. I take a statin—and ezetimibe—every day. No symptoms. No cardiac history. Just an honest read of the evidence. Here's what I found—and why I stopped waiting for a reason to act.




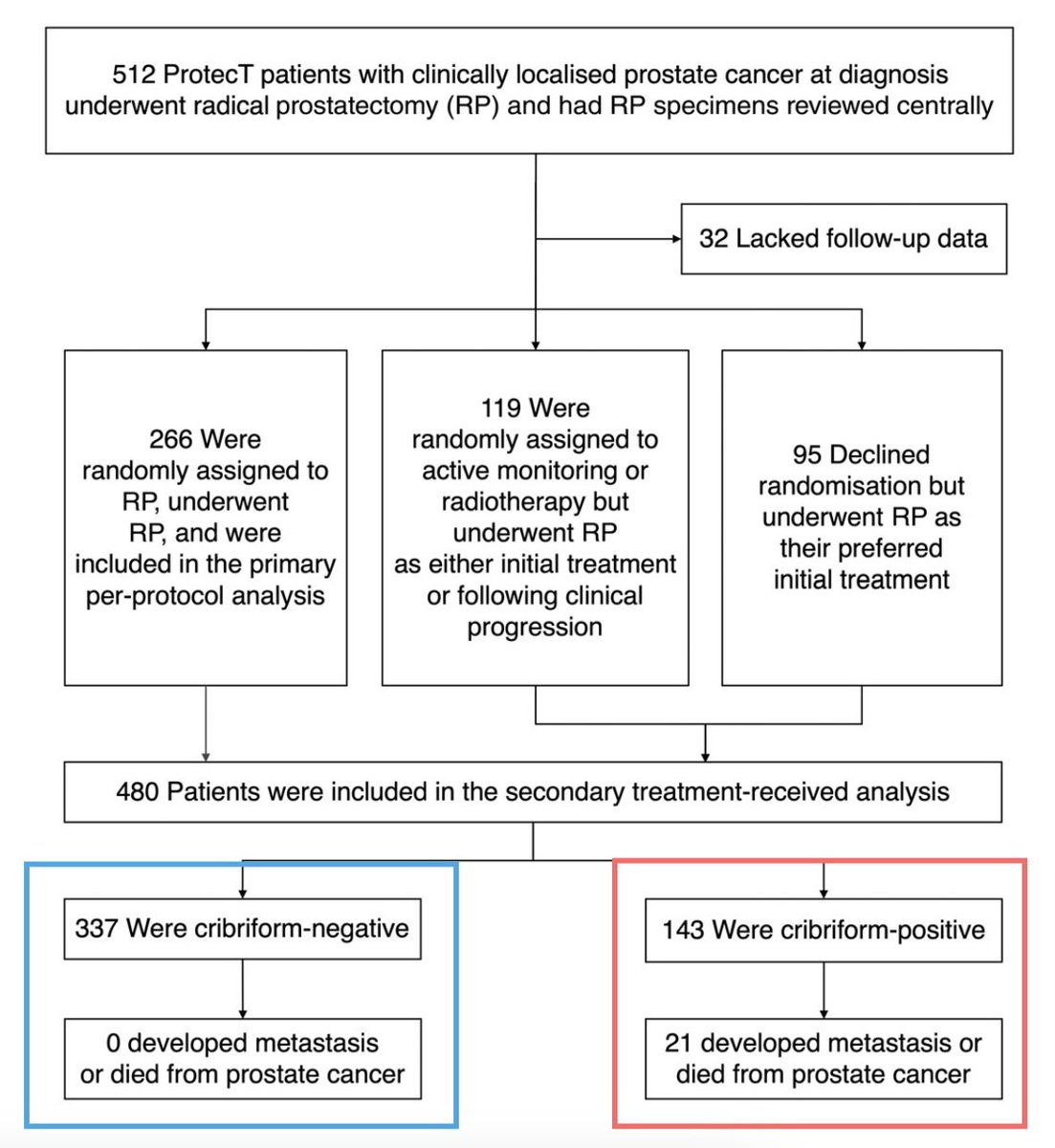
@ShakeKumarMD @TylerSbrt7 @davidjeinstein @DrVMuralidhar @BIDMCUrology Sadly even today we can’t be confident that cribriform status was assessed in biopsy reports that don’t explicitly mention the presence/absence of cribriform morphology 🫠 Which makes us review every single Bx even in contemporary pts - despite ISUP mandating this in 2019 (!)



11 ▶️95% of EPE was pattern 3 extending beyond capsule ❌30% of SVI had crib+ cells in SV Implications: ⛔️Obsessing about EPE on MRI prob. not v helpful ✅We want to detect SVI, GG3, and cribriform‼️ @Adam_Weiner535 @LondonProstate1 @DoctorMargolis @Dr_RaviMadan

Estudio prospectivo comparativo (2020-2022): Aquablation vs HoLEP en HPB. HoLEP mostró mejores resultados en IPSS, Qmax, PVR y función eréctil (IIEF) a 12 meses, pese a volúmenes prostáticos similares. Evidencia clave para LUTS/BPH. pubmed.ncbi.nlm.nih.gov/38722445/



Excellent talk by @drjkaouk on Single Port prostatectomy. Data shows early return to continence compared to multiport, consistent with what we’ve seen with our transvesical single port prostatectomies @RamPathakMD
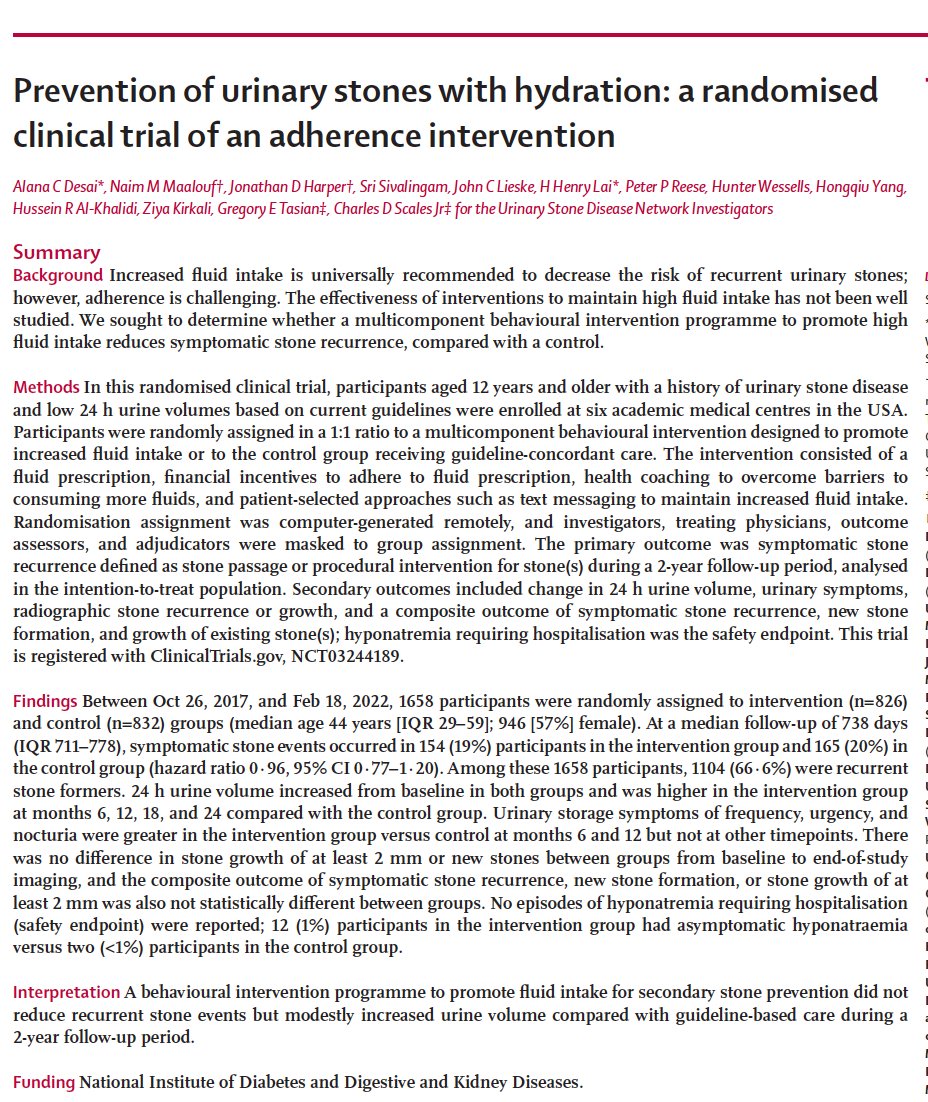




If you've had a kidney stone, you've been advised that the most important thing to prevent another bout is to increase hydration. Now a randomized trial of hydration in over 1600 participants showed no benefit, despite evidence of increase during volume. thelancet.com/journals/lance…