Tweet ghim

#_POCUS
Few tips for learning POCUS for beginners like myself
1- it is very steep learning curve & long journey.
2- pick up one source & keep watching it over & over again. Youtube has lot of them
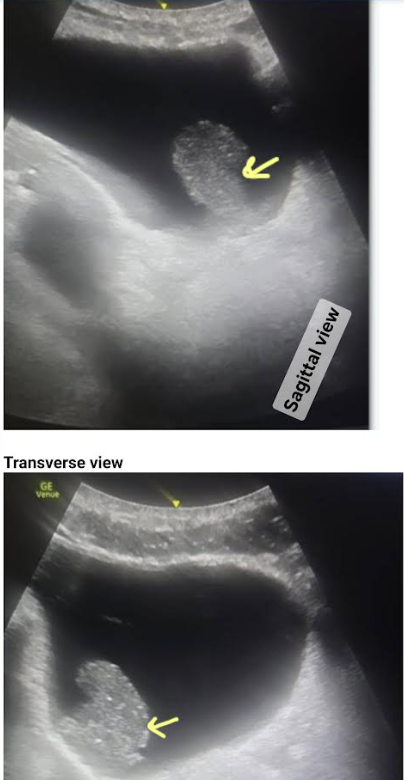
3- POCUS has 3 parts: image acquisition, interpretation & clinical integration
English