Nick Norwitz MD PhD@nicknorwitz
There’s been a lot of engagement and curiosity around the new Ez-PAVE results for intensive lipid lowering. Here are a few observations and some questions worth asking.
First, the headline: intensive lipid-lowering therapy led to a 33% relative risk reduction (HR 0.67) and, more notably, a 3.1% absolute risk reduction in major adverse cardiovascular events (MACE)—including cardiovascular death, heart attack, stroke, revascularization, and hospitalization for unstable angina—over three years.
Pause there. If that effect is real, it’s impressive. But it also raises some important questions.
1. How much of this effect is actually attributable to LDL lowering?
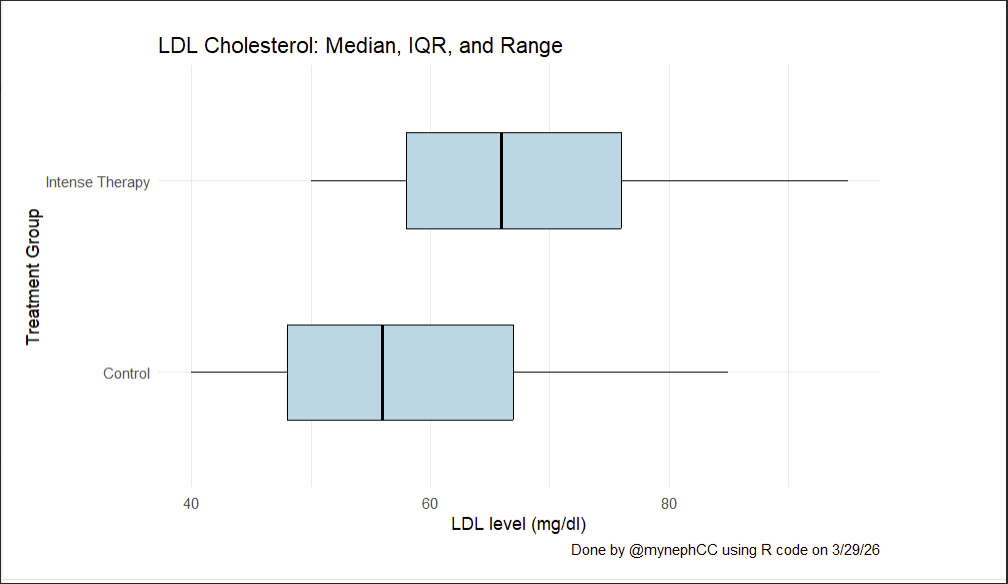
The difference in LDL between groups was modest: a median of 56 mg/dL vs. 66 mg/dL.
A ~10 mg/dL delta leading to a >3% absolute reduction in MACE over three years is a large effect size—and not one that feels immediately biologically intuitive.
Is there a threshold effect at play? Something nonlinear about risk reduction at lower LDL levels? Or are we seeing effects beyond LDL itself?
2. Is there something unique about the population?
This was a South Korean cohort. Could there be population-specific factors—genetic, environmental, or metabolic—that make individuals more responsive to modest lipid reductions or to the pleiotropic effects of the therapies used?
3. Who actually benefited?
One under-discussed point: the benefit appears to be driven almost entirely by men.
There was no clear evidence of benefit in female participants (HR 1.22)
Yes, the cohort was male-skewed—but if you look at the hazard ratios, the signal is coming from men. That raises an important caution: these results may be prematurely generalized to populations (particularly women) where the data simply don’t support it.
At present, the strongest evidence here applies to South Korean men. Question: Does the effect generalize?
4. What about the therapies themselves?
“Intensive lipid lowering” wasn’t a single intervention—it included a spectrum of medications, each with distinct mechanisms and potential off-target effects. All of these should be considered for management of any individual patient… obviously.
This includes off-target “good” effects, and off-target “bad” effects.
As one case in point of additional “good” effects, take ezetimibe. Early data suggest potential neuroprotective benefits entirely independent of lipid management. I'm choosing to highlight a examples of a non-lipid pleiotropic "good" effect so no one can accuse me of 'cherry-picking,' but the point remains: this is more than a "lower LDL is better" story. It always was. It always will be.
It’s sad, honestly, that when data like these come out the gut reaction is to shallowly wave a “lower is better” flag and attack the “LDL deniers” and “keto-zealots” in the name of virtue-signaling evidence-based medicine. It’s almost cultish behavior. In many cases, the shallowness of commentary reveals an almost intentional ignorance or, at minimum, a deficit in curiosity of what's actually going on in different human populations.
Bottom line: These are interesting and potentially important data. They deserve thoughtful discussion—not dismissal. But simply waving the flag of “lower is better” isn’t a sufficient or rigorous interpretation of what’s actually going on here.
We should be asking better questions.
@realDaveFeldman @ApoDudz @AdrianSotoMota