
@theproof @reallyoptimized @__Jon_Power__ @YouTube Since Cleerly is an automated analysis that doesn’t require human input, why does blinding matter? And why would Cleerly have any bias to push the results to look worse?
English
Jason Infeld, MD
1.2K posts
@infeldMD
Cardiologist/Stern Cardiovascular Foundation/Director of Echocardiography/Director of Lipid Clinic



@ZKForTre He's using the word correctly, is all.

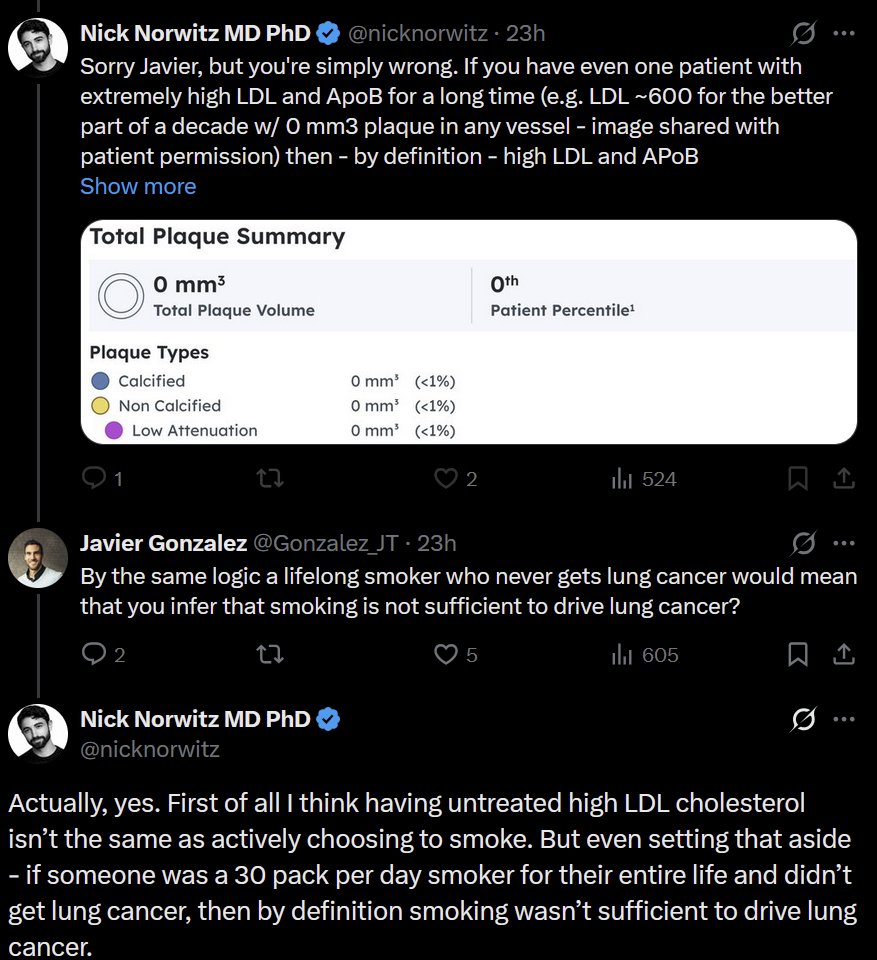
Just amazing how corrupt the academic system is, even in so-called independent testing facilities such as Cleerly, who fraudulently unblinded the lean mass hyperresponders study data and then altered it, making it appear as if there was an increase in cardiovascular plaque when in fact there was an overall reduction in the entire cohort. Just amazing as they were being paid to do an objective job, but for some reason they decided to corrupt the data for their own purposes. These people should be sued into oblivion, and hopefully will be. So again to everybody who thinks that ketogenic and ketogenic carnivore diets with so-called elevated LDL and total cholesterol but high HDL, low triglycerides, and massive improvement in every other biomarker and physical marker are somehow at risk for developing cardiovascular disease, the evidence is in: ketogenic diets, like a carnivore diet, reduce arterial plaque, even with elevated LDL and ApoB. And in fact, both data sets, even the corrupted one, show that there is NO association whatsoever between plaque progression and LDL or ApoB. None. Zip. Zilch. Nada. Sorry cholesterol bros, you're wrong again!


It is healthy to consume saturated fat in the diet. It is healthy to consume saturated fat in the diet. It is healthy to consume saturated fat in the diet. It is healthy to consume saturated fat in the diet. pubmed.ncbi.nlm.nih.gov/36059207/

It can be true that LDL levels and LDL-lowering are associated with heart disease outcomes, much like fever and temperature-lowering are associated with outcomes in sepsis. Lowering fever may help a patient feel better or even marginally improve survival, but it doesn’t mean the fever was the cause or that suppressing it treats the root problem. Fever is a marker of the underlying infection; LDL may likewise be a marker of potential harm for untreated metabolic disturbance. What’s been ignored in this analogy is the real “infection” driving cardiovascular disease: insulin resistance and metabolic syndrome. Treating LDL alone while neglecting metabolic dysfunction is like treating sepsis by giving acetaminophen but ignoring antibiotics. You might temporarily change a number, but you’re not addressing the root cause of the disease process. Until we confront insulin resistance, hyperinsulinemia, and poor metabolic health directly, we’ll keep mistaking correlation for causation, lowering LDL as if it were the infection itself, while the true pathogen, metabolic dysfunction, continues to rage unchecked.

RFK Jr is wrong. Like usual. Beef tallow is not healthier than seed oils. RFK Jr is immune to evidence. DECADES of DATA: Polyunsaturated fats in seed oils reduce risk of heart disease & atherosclerosis compared to saturated fats in beef tallow. Watch: youtu.be/bGrfbs8qxPo?si…
Do not consume dietary supplements with the following ingredient(s) even if prescribed by a legit doctor (these are well known liver toxic agents with additional risks, some fatal): - green tea extracts - curcumin - black cohosh - ashwagandha - giloy (tinospora cordifolia) - scutellaria (chinese skull cap) - aristolochia indica - bitter orange - valerian - aloe vera - bakuchi (psoralea corylifolia) - garcinia cambogia - ginko (also increased risk of bleeding) - ginseng (mostly heart related side effects) - gugulipid (guggulu) - kava - comfrey - sweet flag (acorus calamus)


@Lpa_Doc Had a huge LPa increase when I doubled my Crestor to 40mg. Added repatha and lowered my Crestor to 20mg - my LPA dropped 300 points. Now trying 5mg Crestor (with repatha). Could statins affects on LPA be different for everyone? My Dr. has never seen statin affect LPA this much.


🚩"Detox" and "cleanse" are some of the biggest red flags for BUNK! 🚩 No. No. No. No. No. No. No. No, they do not work.

