Action for Health retweetledi

“I have every lawyer in town bowing gratitude to me for the work they got out of that law.” - Pete Stark
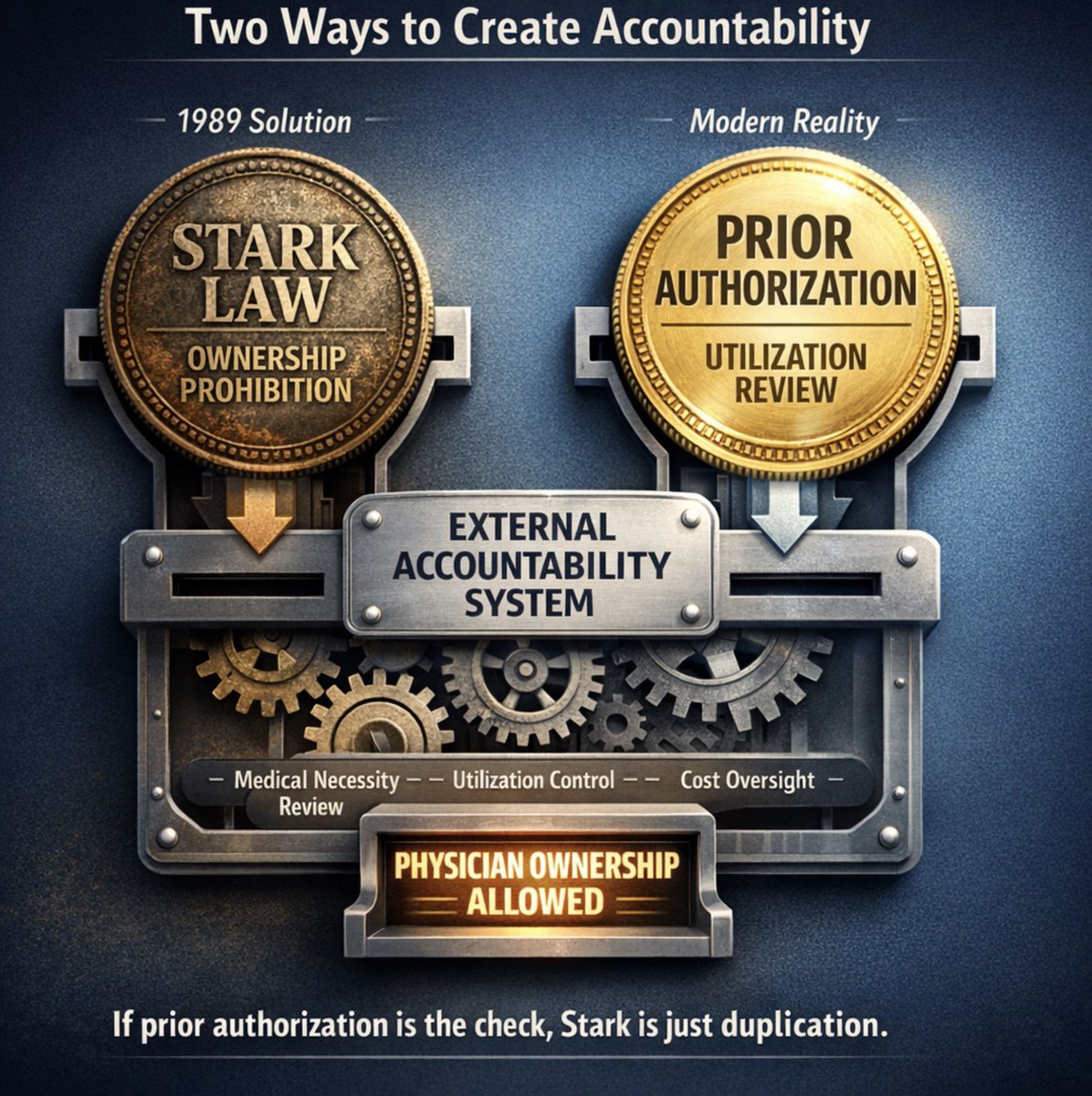
The core argument for the Stark Law has always been that without regulation, physicians with financial interests in referral destinations will over-utilize, and there is no external check to stop them.
That argument may or may not have had merit in 1989. Regardless, it does not hold in a world of 50 million annual prior authorization requests.
Prior authorization is prospective utilization review. Before a high-cost imaging study, surgical procedure, or specialist referral is approved, a payer independently evaluates medical necessity. That is precisely the external accountability check Stark was designed to substitute for. When qualified utilization review exists, the foundational justification for the Stark prohibition disappears.
Researchers at Johns Hopkins made this case in JAMA Health Forum, proposing that self-referral should be permitted within capitated, risk-adjusted payment programs, including Medicare Advantage, because managed care tools already address the overutilization concern Stark was written to solve. A CMO at Temple Faculty Physicians arrived at the same conclusion independently, telling Becker’s this week that if a process is structured to address what patients need without a fee-for-service reward driving it, there is no reason to focus heavily on Stark restrictions.
Clinical leaders and peer-reviewed research are pointing to the same answer that the accountability mechanism should be the utilization review process, not a 35-year-old ownership prohibition.
For any service subject to prospective prior authorization or qualified utilization review, physician ownership of the referral destination should qualify for a Stark exception. This satisfies the desire for an external check making Stark redundant.
For physician-owned hospitals, a conditional pathway makes sense. Facilities that subject their procedures to Medicare Advantage utilization review would be able to add all MA plan cases to their facility. If they want full access to the traditional Medicare population, participating in CMS’s own WISeR accountability model should qualify for a conditional exception to the 2010 ban.
These are rational substitutions of modern accountability tools for an outdated and overly burdensome regulatory framework. CMS already operates the infrastructure to fix the problem. We just need Congress or CMMI to recognize it.
English