Austin Baraki, MD retweetledi

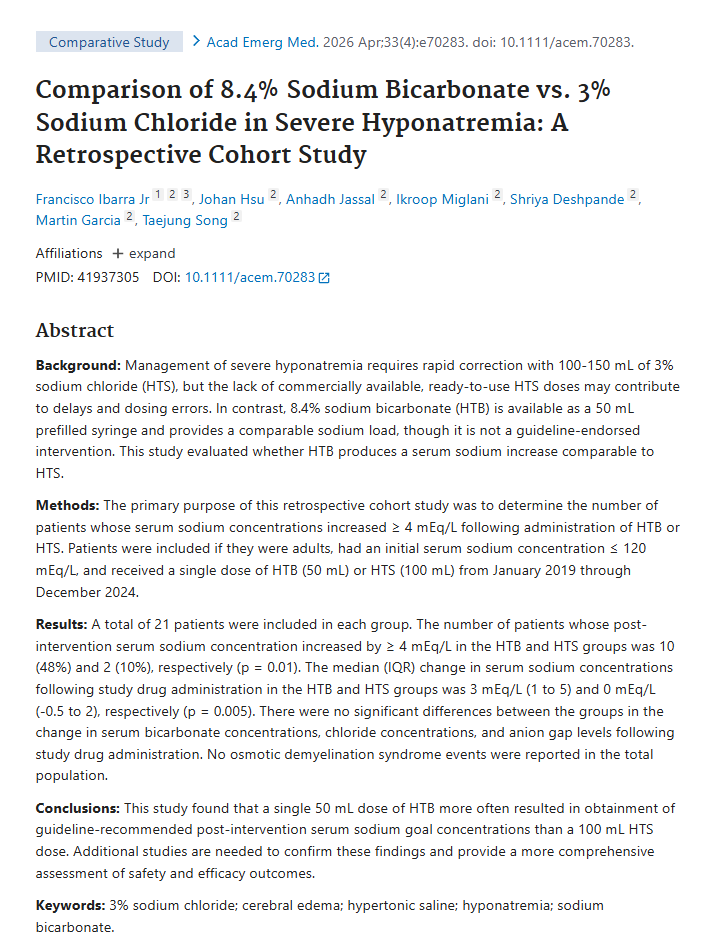
Cool study comparing 50 ml of bicarb vs 100 ml of 3% HTS for hyponatremia. @pulmcrit was talking about this forever ago, nice to see someone do a study on it
bit.ly/4cgLTSu
English
Austin Baraki, MD
3.2K posts
@AustinBaraki
Internist, FACP, Clinical Assoc Prof / Coach @BarbellMedicine / Doc @joinvineyard / Trained @evmsedu @uthsaim



Semaglutide in Patients With Schizophrenia, Prediabetes, and Obesity 🚨 1. Semaglutide significantly improved insulin sensitivity, reduced insulin resistance, lowered fasting glucose, and promoted substantial weight loss in patients with antipsychotic-induced metabolic disturbances. 2. Weight loss partly mediated the metabolic improvements, while β-cell function remained largely unchanged. 3. These findings support semaglutide as a potential strategy for mitigating metabolic dysfunction in this high-risk population. Paper: 👇diabetesjournals.org/care/article/d…




Took me 10 months to unfat myself and I took no Reta. Learned a lot about myself along the way and endured the power of discipline. It sucks but much more rewarding than taking a fat drug or peptide.





1/3: Systematic review of 36 studies on GLP-1 RA and GLP-1/GIP agonist exposure in pregnancy and lactation. Bottom line: no consistent signal for major congenital malformations with periconceptional/early-pregnancy exposure in adjusted analyses. doi.org/10.1111/dom.70…





High meat consumption linked to 55% lower dementia risk in genetic risk group. New study finds older people carrying the APOE ε4 Alzheimer’s risk gene did not experience the expected cognitive decline if they consumed relatively large amounts of meat.










classic teaching: cirrhosis + upper GI bleed = antibiotics for everyone. But how strong is the evidence behind that practice? This Annals of Emergency Medicine Systematic Review Snapshot highlights a Bayesian meta-analysis of 14 randomized trials examining antibiotic prophylaxis in cirrhotic patients with upper GI bleeding. The analysis raises important questions about duration of therapy, while also reminding us about the limitations of older, heterogeneous trials and potential bias in the data. 📚 The takeaway: worth reading, worth discussing, and worth scrutinizing the methods before changing practice. Check out the full Systematic Review Snapshot in Annals of Emergency Medicine and decide for yourself. Reference: Prosty C, Noutsios D, Dubé LR, et al. Prophylactic antibiotics for upper gastrointestinal bleeding in patients with cirrhosis: a systematic review and Bayesian meta-analysis. JAMA Intern Med. 2025;185:1194-1203. Discussed in: Annals of Emergency Medicine Systematic Review Snapshot. #EmergencyMedicine #MedEd #FOAMed #EvidenceBasedMedicine #AnnalsOfEM