Sabitlenmiş Tweet

Dr. Omene MD, PhD
821 posts
@DoctorOmene
Neurologist → Neuro-oncologist | Prof @UAlberta | Neuroscience x Oncology x AI | Cancer metabolism • Clinical trials • Some pop culture & millenial nostalgia

The baby girl’s reaction when she saw a train for the first time 🥹

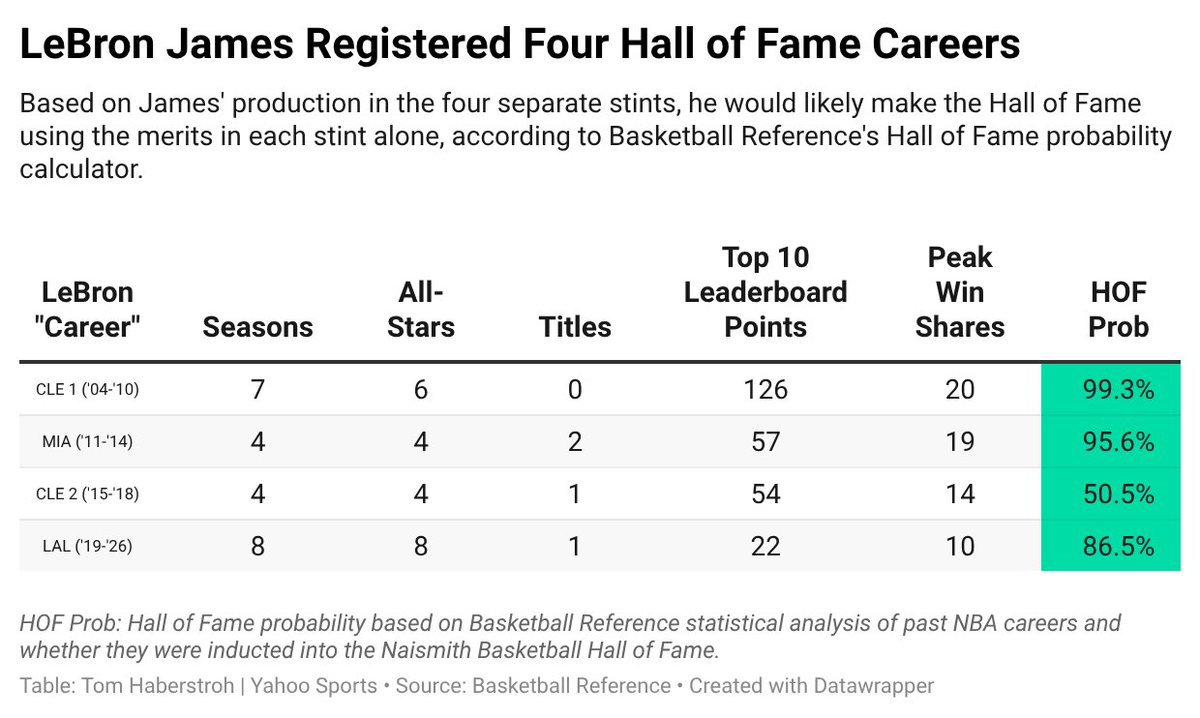
NEW @YahooSports: If last night was truly LeBron James’ final game as a Laker, he’ll walk away knowing he had a Hall of Fame career *based solely on his 8 Lakers years.* LeBron has now stacked 4 HOF careers, and I shared all the data to prove it: sports.yahoo.com/nba/article/ki…





In a phase 1–2 study of daraxonrasib, treatment-related adverse events of grade 3 or higher occurred in 30% of patients with previously treated RAS-mutated pancreatic cancer, and up to 35% of patients had an objective response. Full study results: nej.md/4f7xfhX Science behind the Study: Advances in RAS Therapeutics for Pancreatic Cancer nej.md/4neOTCE




Sobering paper on aging Argues that basically every intervention known to extend lifespan only does so by preventing obesity. In other words, being lean and fit is not just 90% of slowing aging, but 100%. sciencedirect.com/science/articl…


🫁 Lung cancer is no longer just about treating disease, it’s about intercepting its evolution! aacrjournals.org/cancerdiscover… This AACR roadmap lays out the shift: ▪️ From late-stage care → early detection & prevention ▪️ From static biology → dynamic tumor evolution ▪️ From single targets → multi-omic integration ▪️ From relapse treatment → MRD-driven intervention The future? Anticipate. Intercept. Adapt. @OncoAlert @OncoReporte @myESMO @_SEOM @LungCancerRx @Lung_Cancers

A PET scan finds cancer by injecting you with radioactive glucose and watching where it goes. The tumour lights up like a Christmas tree. The healthy tissue does not. The machine that diagnoses your cancer is, mechanically, a sugar detector. The thing it is detecting is the thing the cancer is eating. Your oncologist will then hand you a leaflet recommending complex carbohydrates as part of a balanced recovery diet. Read that twice.