
English
RaiderOS
121 posts


@Donna7563291556 They also have very serious side effects Lowering cholesterol is also not beneficial







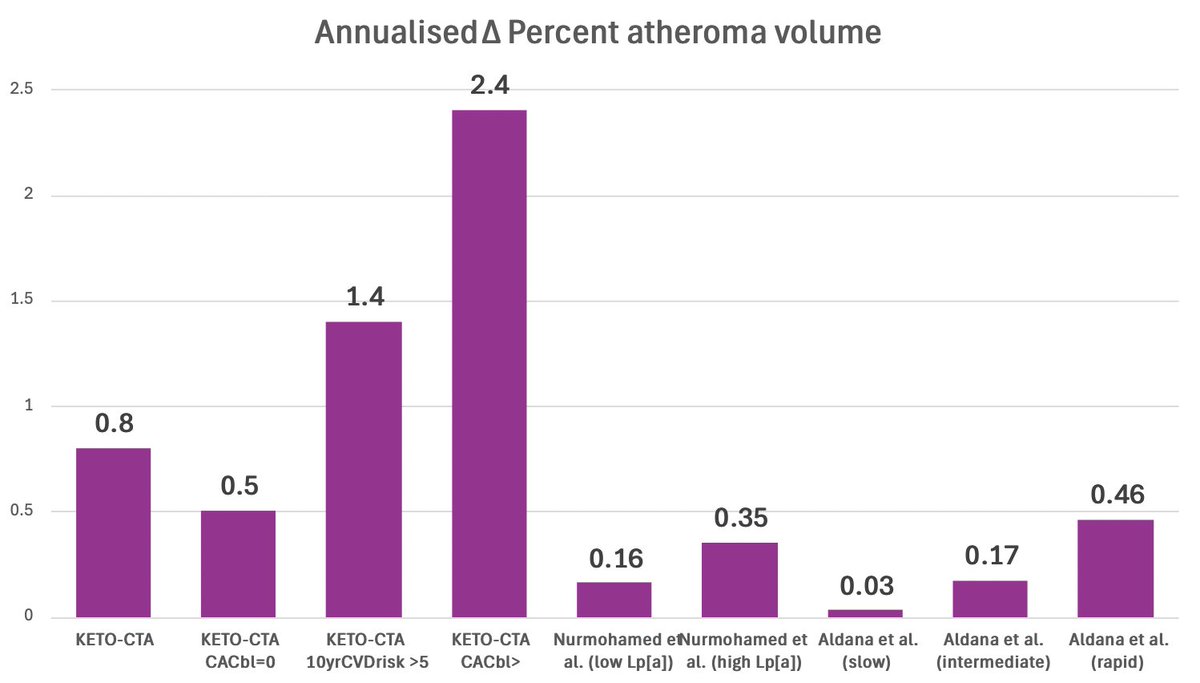
I’ve been watching with amusement that some people seriously believe that CCTA is an imaging tool with outcome figures so precise that data from different machines, software, and evaluating person are quantitatively comparable to the extent that 18.8 mm3 from one study is exactly 57 % higher than 12 mm3 from another study. Not to mention differences between patient populations in various studies. Also not to mention the total lack of thresholds in PAV changes for clinical significance. (Below is the difference between software only.) That’s straight funny, and clearly shows that people love to argue without doing even the minimum amount of background reading necessary.
@SBakerMD I'm wondering if there is evidence that keto helps reduce plaque.

As expected, after reading the paper, the contents of every tier on that hierarchy, as well as the tiers themselves, are pulled completely out of Nina's ass. The evidence for this is actually worse than the evidence for the original USDA food pyramid that she criticizes. 🙄





Avalanche9000 is the upgrade web3 gaming has been waiting for. 🎮 Dedicated L1s Smoother gameplay for players, with no lag or fee spikes. Developers get customizable, scalable chains for their games. 🎮 Interoperability Gamers can seamlessly transfer assets across chains. Developers reach wider audiences with secure, cross-chain compatibility. 🎮 Developer Experience Faster, less expensive game L1 launches with easier deployment and new tools to get it done. 🎮 Player Economy Instant marketplace transactions and stable infrastructure ensure better in-game experiences. Not to mention the improvements to the C-chain for games that aren’t ready for their own L1 and want to launch there. Taken together, these upgrades are clearing the path for an avalanche of new web3 games.




