Simeng Zhu retweetledi

How do they produce such crazy papers?

English
Simeng Zhu
82 posts
@SimengZhuMD
Radiation oncologist @OSUCCC_James. Medical AI reseacher.





The California Head & Neck Consortium released the first multidisciplinary consensus recommendations on the use of circulating tumor HPV DNA in HPV+ oropharyngeal carcinoma. The panel of 33 experts representing 15 institutions reached strong consensus that a tool like the NavDx® test should be incorporated into routine surveillance. The consensus recommendations also included: Using an option like the NavDx test improves time to recurrence detection vs. conventional surveillance tools, but should supplement these methods, not reduce or replace them. The recommended time for a patient’s first post-treatment test is 3 months. Serial testing should be performed in conjunction with conventional surveillance every 3 months in the first 2 years post-treatment and every 6 months in years 3-5. For patients with a single positive post-treatment test where no clinical or radiographic evidence of disease is present, the best time to repeat the test is in one month. Earlier molecular detection of locoregional or oligometastatic disease should improve outcomes. These recommendations reinforce real-world clinical validation and value of new technologies like the NavDx test in earlier detection of molecular residual disease and recurrence of HPV+ oropharyngeal cancer. Access the full publication here: bit.ly/3MrPgeG #ctHPVDNA #HeadAndNeckCancer #Oncology #MRD #NavDx #CancerSurveillance #hncancer




During the #NRG2025 General Session, @dsmgyo presented the the top accruing NRG sites. Congratulations and thank you to all NRG member sites!
Honored to participate at The James Ambassadors Foundation Fall Celebration. Thanks to our @OSUCCC_James Ambassadors for supporting research. “Precision, Collaboration, innovation, translational research personalization and hope are in the future of cancer care” (@David_Cohn_MD)

Back for the last leg of the PRO sessions - H&N toxicity prevention and radiopharm in the community setting #ASTRO2024 @ShaunaRadOnc





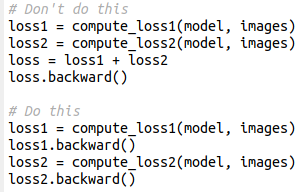
This simple pytorch trick will cut in half your GPU memory use / double your batch size (for real). Instead of adding losses and then computing backward, it's better to compute the backward on each loss (which frees the computational graph). Results will be exactly identical