Kevin Fay retweetledi

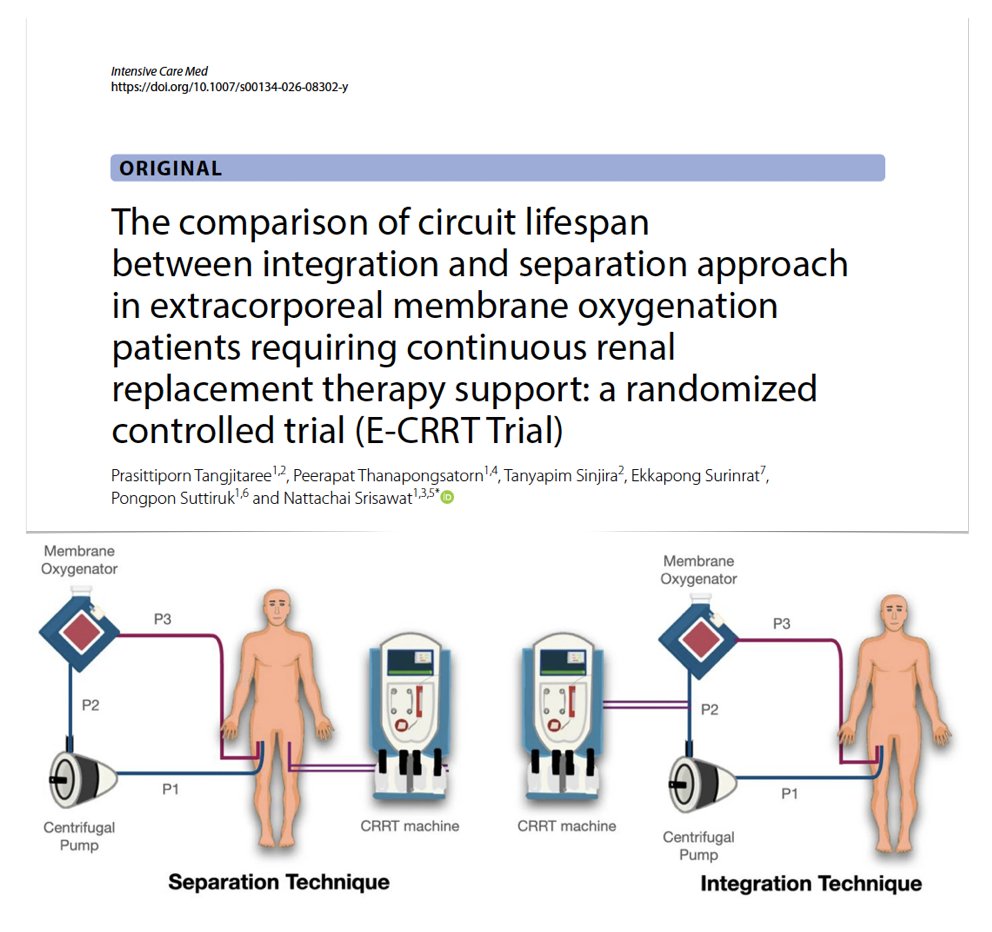
(Circuit) integration or separation approach in #ECMO patients requiring #CRRT? E-CRRT RCT
🔎 80 pts allocated to CRRT/ECMO circuits integration vs separation
⚖️ no significant difference in filter lifespan between integration/separation configurations
🪦 comparable mortality
🫧 no significant differences in serious adverse events, including air embolism
🚨 transmembrane pressure + CRRT machine alarm frequencies similar
#FOAMcc
🔓 rdcu.be/e2FyX
English