@franciscojlk@DrDaleNeedham There may be some overstated point to this post (minor) but the styling is all click-on-me rhetorically optimized, cadenced AI slop ruining #meded
Sweet emojis tho
💉🩺Rapid sequence intubation in 2026: we are no longer “protecting the airway.”
We are managing physiology under extreme stress.
The latest evidence challenges one of the oldest dogmas in critical care.
RSI was designed to prevent aspiration.
But today, the real enemy is often hypoxemia and cardiovascular collapse.
1. Aspiration is no longer the central problem
For decades, RSI was built around one fear: aspiration.
But emerging data suggest:
RSI may not significantly reduce aspiration
It may increase hypoxemia and hemodynamic instability
The paradigm is shifting:
👉 From aspiration avoidance → to physiologic optimization
2. First-pass success is everything
Every additional attempt increases:
Hypoxia
Hemodynamic collapse
Mortality
Modern RSI is built around one goal:
Get it right the first time.
That means:
Videolaryngoscopy first-line
Stylet routinely
Team choreography, not improvisation
3. Preoxygenation is now a therapeutic intervention
Not just a step—a determinant of survival
NIV > face mask
HFNO as adjunct
Semi-upright positioning
And one key shift:
👉 Gentle ventilation is no longer taboo
Done correctly, it reduces hypoxemia without increasing aspiration risk.
4. Hemodynamics matter more than ever
Up to 40–50% of patients experience peri-intubation instability.
The modern approach:
Avoid propofol in unstable patients
Favor etomidate or ketamine
Consider prophylactic vasopressors
Fluid loading?
Not routinely beneficial.
5. Cricoid pressure: from dogma to doubt
No clear benefit in preventing aspiration
May worsen laryngoscopy and ventilation
Current thinking:
👉 Use selectively, or not at all
6. RSI is no longer a rigid protocol
It is now:
Patient-specific
Physiology-driven
Team-dependent
With tools like:
Gastric ultrasound
POCUS-guided decisions
Structured airway protocols
7. The real determinant of success: human factors
Preparation, communication, and coordination matter as much as drugs.
Because in critical care:
The airway is not just anatomy.
It is a moment of systemic vulnerability.
🤓Final message
RSI has evolved:
From speed → to precision
From protocol → to physiology
From individual skill → to team performance
And ultimately:
The goal is no longer just to intubate.
It is to intubate without killing the patient.
📃Reference
Boulos NM et al. Anaesth Crit Care Pain Med. 2026. doi.org/10.1016/j.accp…
@IM_Crit_ Shit article barely grazes the real problems and focuses on cheap points already beaten to death in mainstream media. Basterdization of EBM, abandonment of physiology and critical thinking, algorithms tha don’t require personal understanding and can be followed by nondoctors
@DogsMumm@SikandarAdwani The history is combined with the physical examination. No doctor would look at a robust patient and nod and agree with a self serving family member describing him as frail. This is still a hands on field
@SikandarAdwani “Frailty” described by family members might not meet the patient’s own assessment. It’s a very subjective term. Sometimes people make self serving decisions.
Teaching point for daily ICU practice
A patient is admitted after a cardiac arrest. The heartbeat is restored. The initial brain scan is not catastrophic. He is on a ventilator and receiving standard intensive care.
While speaking to the family, we learn that before this event he was slow, needed help with daily activities, and had limited physical strength. Someone describes him as frail.
From that point, something quietly changes in our thinking. Prognosis starts sounding guarded.
Conversations slowly move from treatment to limitation of care. Life support is withdrawn, often not because of clear brain death, but because the overall picture feels poor.
This raises an important question. Did the patient die because frailty made recovery impossible, or did frailty influence how we expected the outcome to be?
A recent editorial in Intensive Care Medicine by Boulet and Muller reminds us to pause here. Frailty is clearly associated with worse outcomes after cardiac arrest. That is true. But frailty is not the same as certainty. Many studies include only selected patients who were already considered suitable for intensive care. Even among them, withdrawal of life support happens more often in frail patients, sometimes for reasons other than definite neurological injury.
This can create a cycle. Frailty lowers expectations. Lower expectations lead to earlier withdrawal of treatment. Withdrawal then confirms the poor outcome.
The teaching point is simple. Frailty is one piece of information. It is not a diagnosis and it should not be the decision. Frailty should help us have better conversations with families about values and goals. It should not silently push us toward giving up too early.
Good intensive care is not only about predicting who will survive. It is also about being aware of how our own perceptions influence decisions.
Sometimes the most important step is to slow down and reflect.
Based on editorial by Boulet N and Muller L, Intensive Care Medicine, 2025.
#NeuroICU#Neurotwitter#Medtwitter
@aclong111@SikandarAdwani Truth. And frailty is huge contributor to baseline health. It’s the depleted savings account where health points needed to pay for recovery from critical illness were stored.
A key lesson from OHCA: early neuroprognostication is unreliable and risks becoming a self-fulfilling prophecy. Baseline health matters, but unless families prefer otherwise, waiting for full multimodal prognostic data is critical, because premature conclusions can shape decisions in ways that can’t be undone.
@SikandarAdwani Frailty, ICD diagnostic code R54, is probably the most underdressed and ignored diagnosis in critical illness, to imply that it should get less frequently acknowledged in prognostication, rather than more than it currently does, is an awful approach to medicine. Fully disagree.
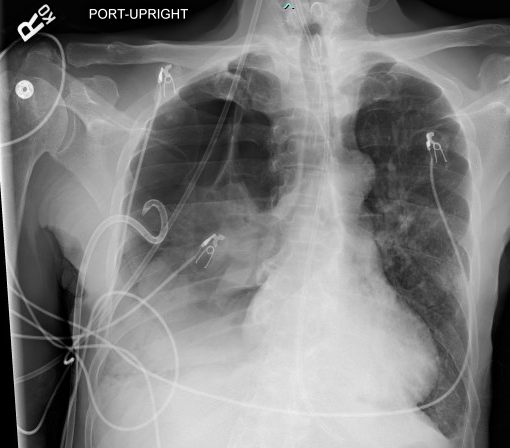
@rbarbosa91@pabloperezc Also doesn’t account for some intrathoracic kinks that can form functional one way valves. Also a 14F CT is no match for a 7.5mm ETT if the lung defect is big enough
@pabloperezc In these cases, we just didn’t want more drama.
Also, when you flush it, I think it tends to unclog only a single side hole, which makes it very prone to happening again. I might try to demonstrate that with one of my experiments with Jell-O or something.
Nowadays we mostly place the 14 Fr Wayne chest tubes, and the data generally support this, but remember they can still fail.
Here are two instances where a 14 Fr chest tube became clogged, and a large pneumothorax resulted. Both had larger tubes placed and the PTX resolved.
@NEJM Guessing $5mil equivalent dollars and 50,000 man hours was spent proving that a single intervention replaced by a near equivalent intervention for a 4 hour period don’t move the coarsest of outcomes in critical care. Next noninferiority trial of scrubs v shirts and ties.
In the EVERDAC trial involving patients with shock, results for death at day 28 indicated that management without early arterial catheter insertion was noninferior to early catheter insertion. Full trial results and Research Summary: nej.md/3LmOO0D
ICU community is like: “there are no positive studies, we need to stop focusing on outcomes like mortality”.
Andromeda-Shock2 shows reduction in vital support and in a well done RCT that is highly generalizable to most septic patients worldwide.
ICU community is like “well where are the KM curves showing mortality reduction…”
I guess no winning eh?
@venkmurthy It’s incredible that time and gold got devoted the answering the question of whether delaying an arterial line insertion by 4 hours increases all cause mortality.
When I first started in medicine idea of not using arterial line in ICU patient was seen as crazy
I remember asking why we couldn't just use cuff for a few hours on particularly busy 30 hour call shift
Now we know that cuff BP would've been fine because of an amazing & bold RCT
nejm.org/doi/full/10.10…
@austincamp This isn’t new per BALANCE. It’s been evidence based for years. Anyone giving 10–14 days post source control without some compelling reason is actually committing malpractice
An ICU rounds convo…
Me: Can we reduce duration of ABX to 7 days?
Them: Isn’t 10-14 more appropriate for gram (-) bacteremia?
Me: Per the BALANCE trial, a 7-day course of ABX was non-inferior to 14 days.
Them: Is this in guidelines yet?
Me: …
What would YOUR response be??