Dr Chris Huff retweetledi

I want to make explicit the absurdity of this pivot from Norwitz:
He is using a subset of 8 Cleerly scan pairs (setting aside the preposterous level of clinical research violations this involves) to argue that the original 100 pairs, which were burdened by unmanageable levels of intra-assay variance, were invalid. The same test. With less power. But now, since they see less progression, it’s exonerating.
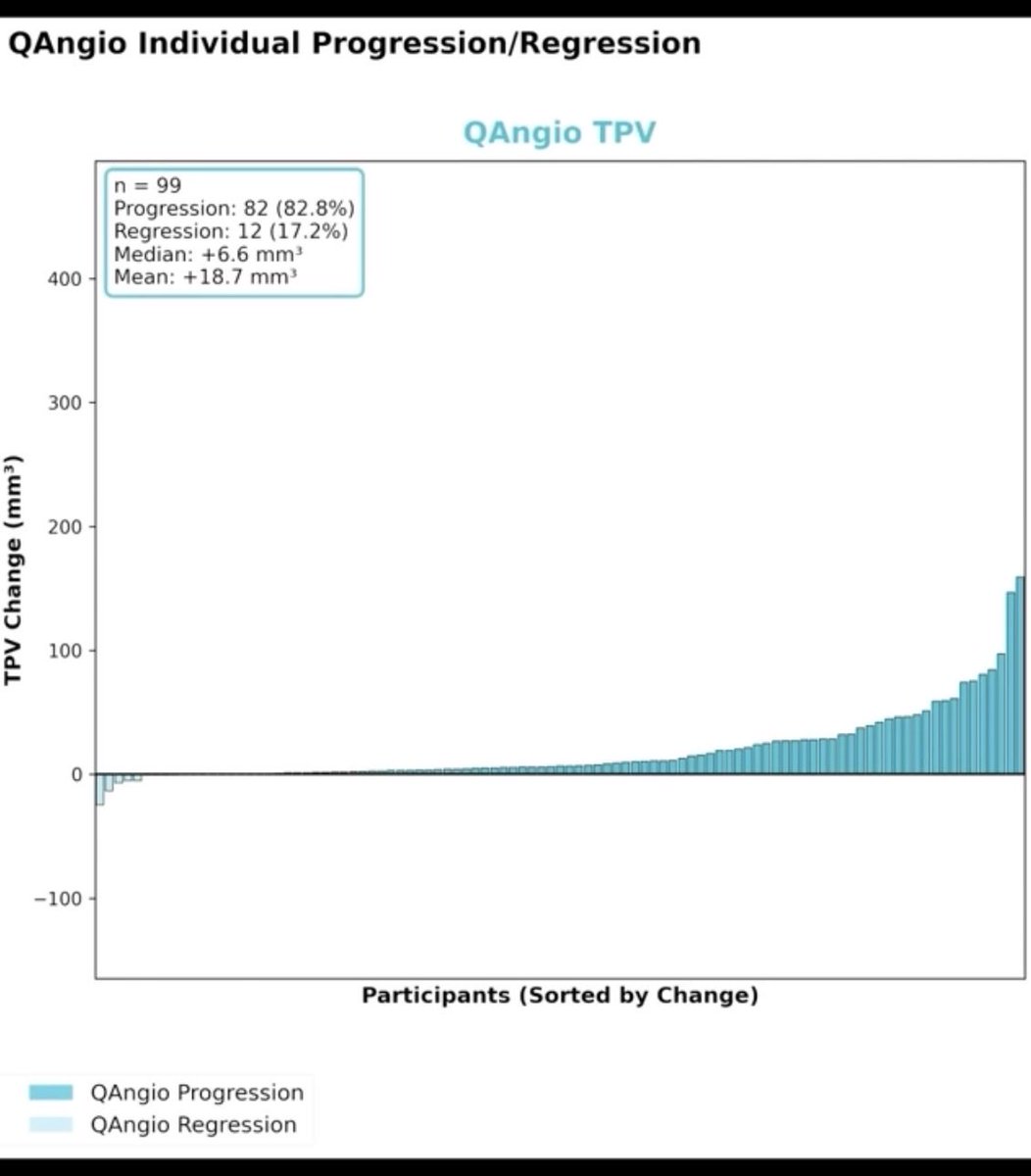
The only appropriate consideration left was to say the methodology was invalid and retract. Put together a new analysis with heartflow or Qangio if you want, but claiming this is exonerating is absurd.
If you had any doubt remaining that this is an exercise of narrative building, you need not have it anymore.
English