@PamelaMasonEP That is one of the reason I switched to stick the vein before cutting down to form the pocket. (Or do a venogram). Impressive lead positioning, but would have been easier from the right.
English
Zoltan Toth,MD
37 posts
@otantot
Electrophysiologist@Texas Cardiac Arrhythmia, Ep fellowship @University of Chicago,









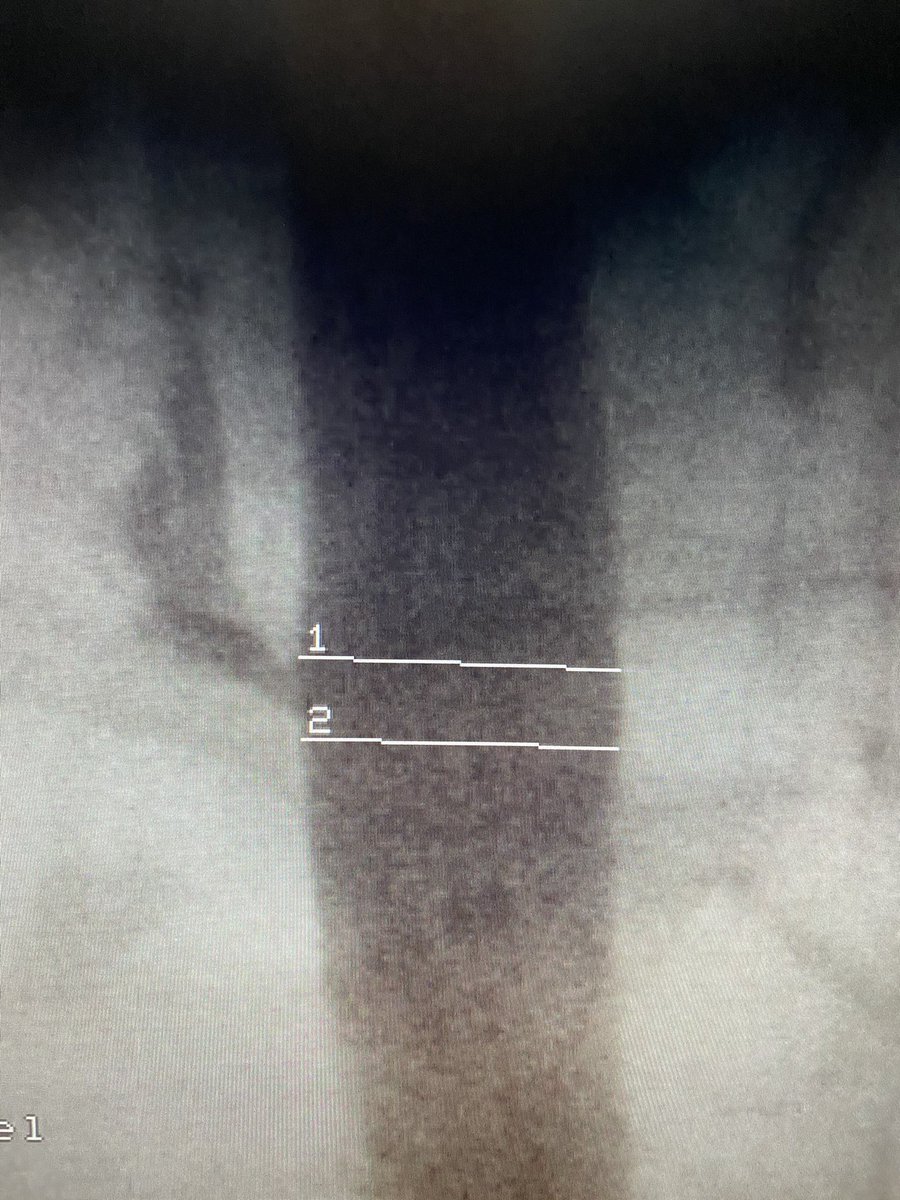


Another case LV lead pulled back now target is occluded. Sleeve tied tight directly to the muscle but then turned to scar. Can't tie directly to the muscle with enough tension to pass tug test without causing necrosis then scar. Tie to the Knot. #EPeeps @narrowQRS @rdschaller