
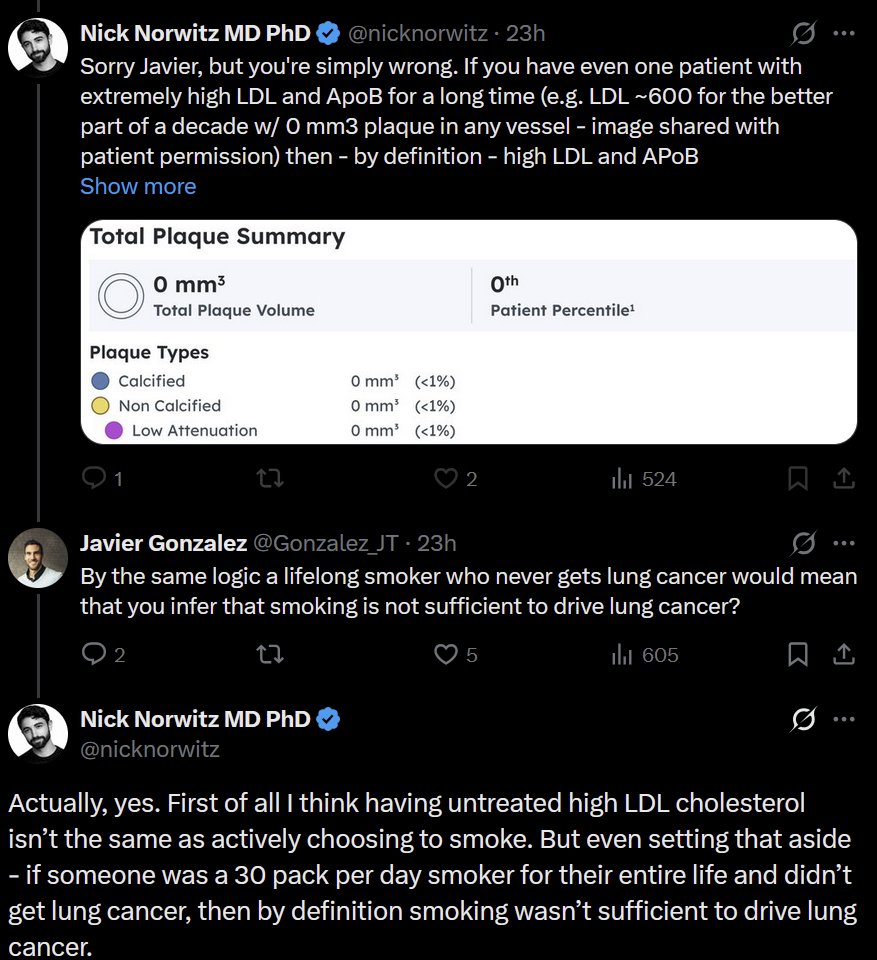
@theproof @reallyoptimized @__Jon_Power__ @YouTube Since Cleerly is an automated analysis that doesn’t require human input, why does blinding matter? And why would Cleerly have any bias to push the results to look worse?
English
Jason Infeld, MD
1.2K posts
@infeldMD
Cardiologist/Stern Cardiovascular Foundation/Director of Echocardiography/Director of Lipid Clinic



@ZKForTre He's using the word correctly, is all.

Just amazing how corrupt the academic system is, even in so-called independent testing facilities such as Cleerly, who fraudulently unblinded the lean mass hyperresponders study data and then altered it, making it appear as if there was an increase in cardiovascular plaque when


It is healthy to consume saturated fat in the diet. It is healthy to consume saturated fat in the diet. It is healthy to consume saturated fat in the diet. It is healthy to consume saturated fat in the diet. pubmed.ncbi.nlm.nih.gov/36059207/

It can be true that LDL levels and LDL-lowering are associated with heart disease outcomes, much like fever and temperature-lowering are associated with outcomes in sepsis. Lowering fever may help a patient feel better or even marginally improve survival, but it doesn’t mean the

RFK Jr is wrong. Like usual. Beef tallow is not healthier than seed oils. RFK Jr is immune to evidence. DECADES of DATA: Polyunsaturated fats in seed oils reduce risk of heart disease & atherosclerosis compared to saturated fats in beef tallow. Watch: youtu.be/bGrfbs8qxPo?si…

We pray for the safety of the patients and the medical staff at Soroka Hospital, which just suffered a direct hit from an Iranian missile. This is a grave violation of international law by Iran, which is launching missiles at Israeli cities with the clear intent to target
Do not consume dietary supplements with the following ingredient(s) even if prescribed by a legit doctor (these are well known liver toxic agents with additional risks, some fatal): - green tea extracts - curcumin - black cohosh - ashwagandha - giloy (tinospora cordifolia) -


@Lpa_Doc Had a huge LPa increase when I doubled my Crestor to 40mg. Added repatha and lowered my Crestor to 20mg - my LPA dropped 300 points. Now trying 5mg Crestor (with repatha). Could statins affects on LPA be different for everyone? My Dr. has never seen statin affect LPA this much.

🚩"Detox" and "cleanse" are some of the biggest red flags for BUNK! 🚩 No. No. No. No. No. No. No. No, they do not work.

