Center for Advanced Imaging and Longevity retweetledi

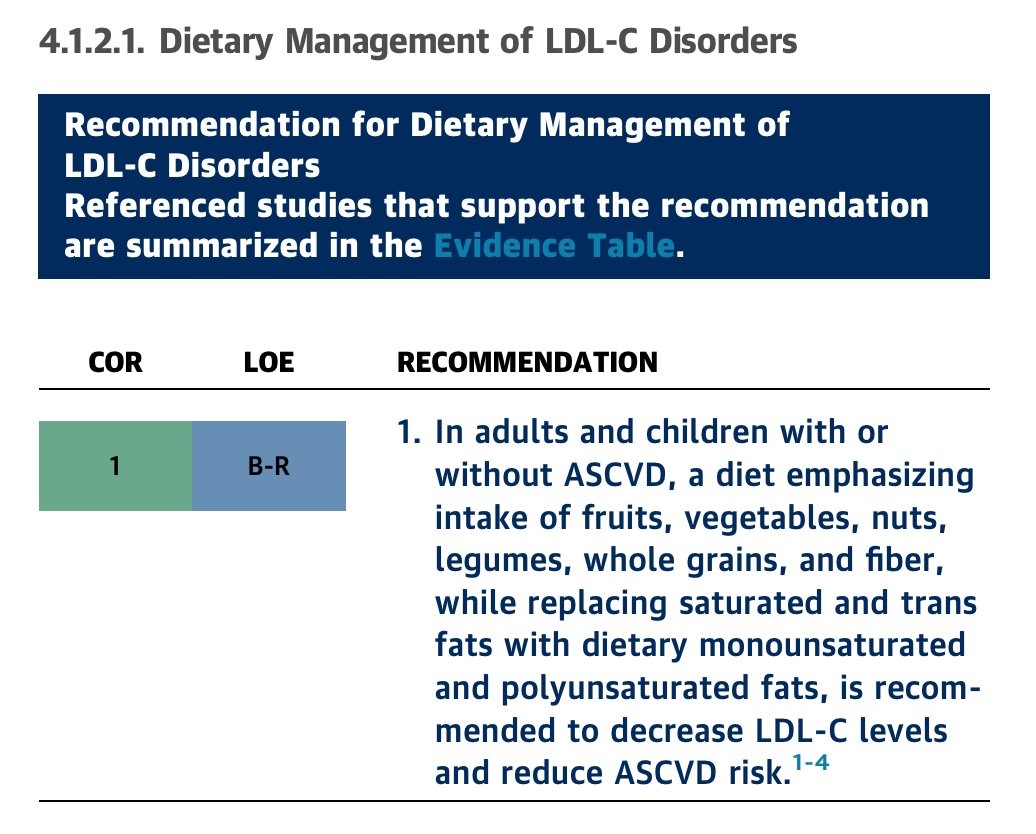
Guidelines reflect evidence, evidence reflects fact. Let's close the gap between facts and clinical practice! Our 2026 ACC/AHA lipid guidelines now promote whole food plant-based vegan diet: ahajournals.org/doi/10.1161/CI…
@ACLifeMed @ACCinTouch @American_Heart @nationallipid @ABCardio1
English