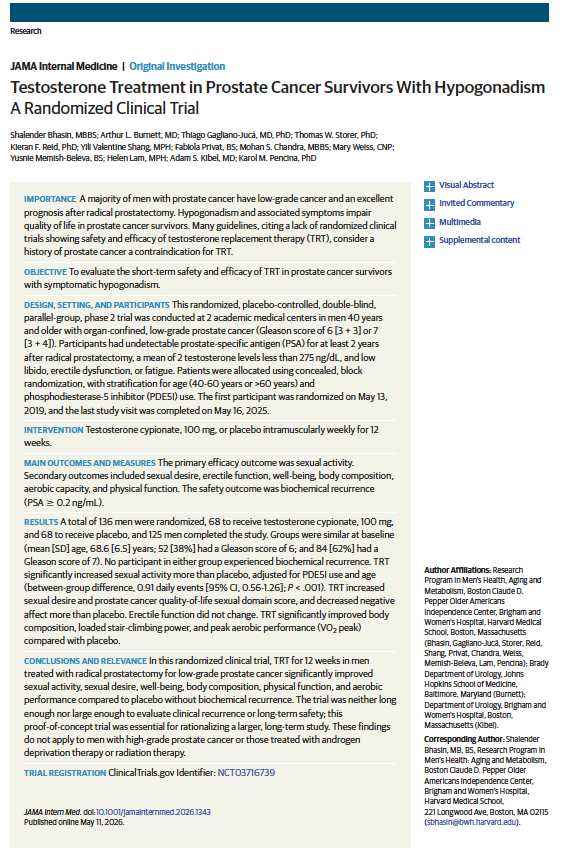
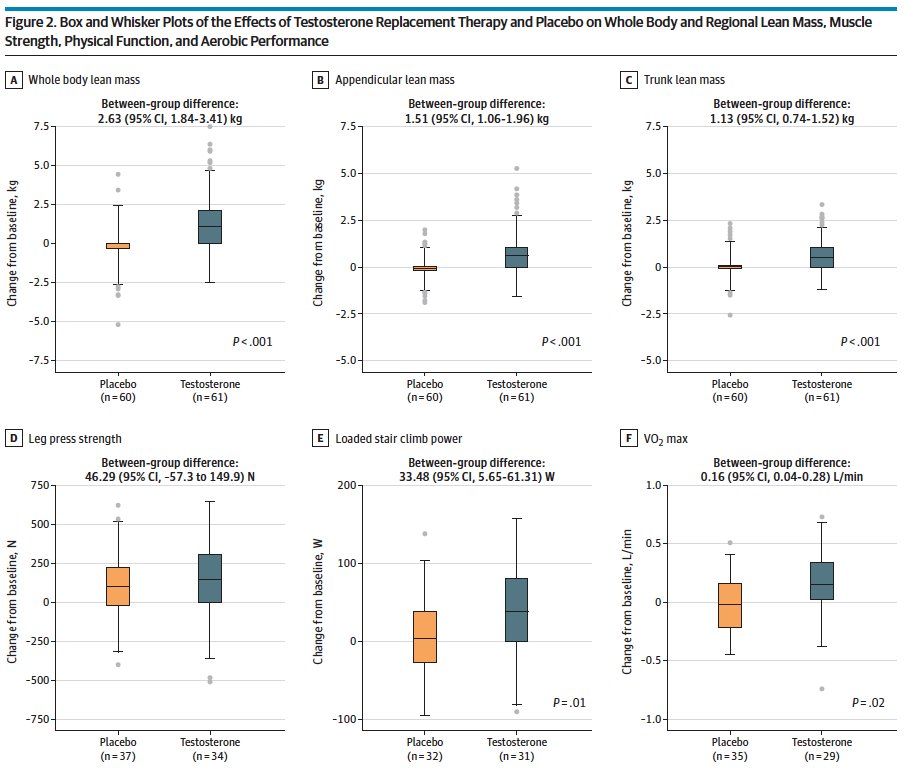
@SPuro88 @Adam_Weiner535 @mubarak_urology @JAMAInternalMed I can’t see a reason TRT should be avoided. Doesn’t data show that TRT is safe even in low risk PCA?
English
Colin Linke, DO
1.2K posts

@ColinLinke
Single Port urologist, owner of Linke Robotics LLC, by way of @LSUHealthNO and @Loyolachicago. All views my own



When anyone orders a non-con CT abdomen for any reason. Truly one of the biggest wastes of time and resources. Along with a PACU lactate.





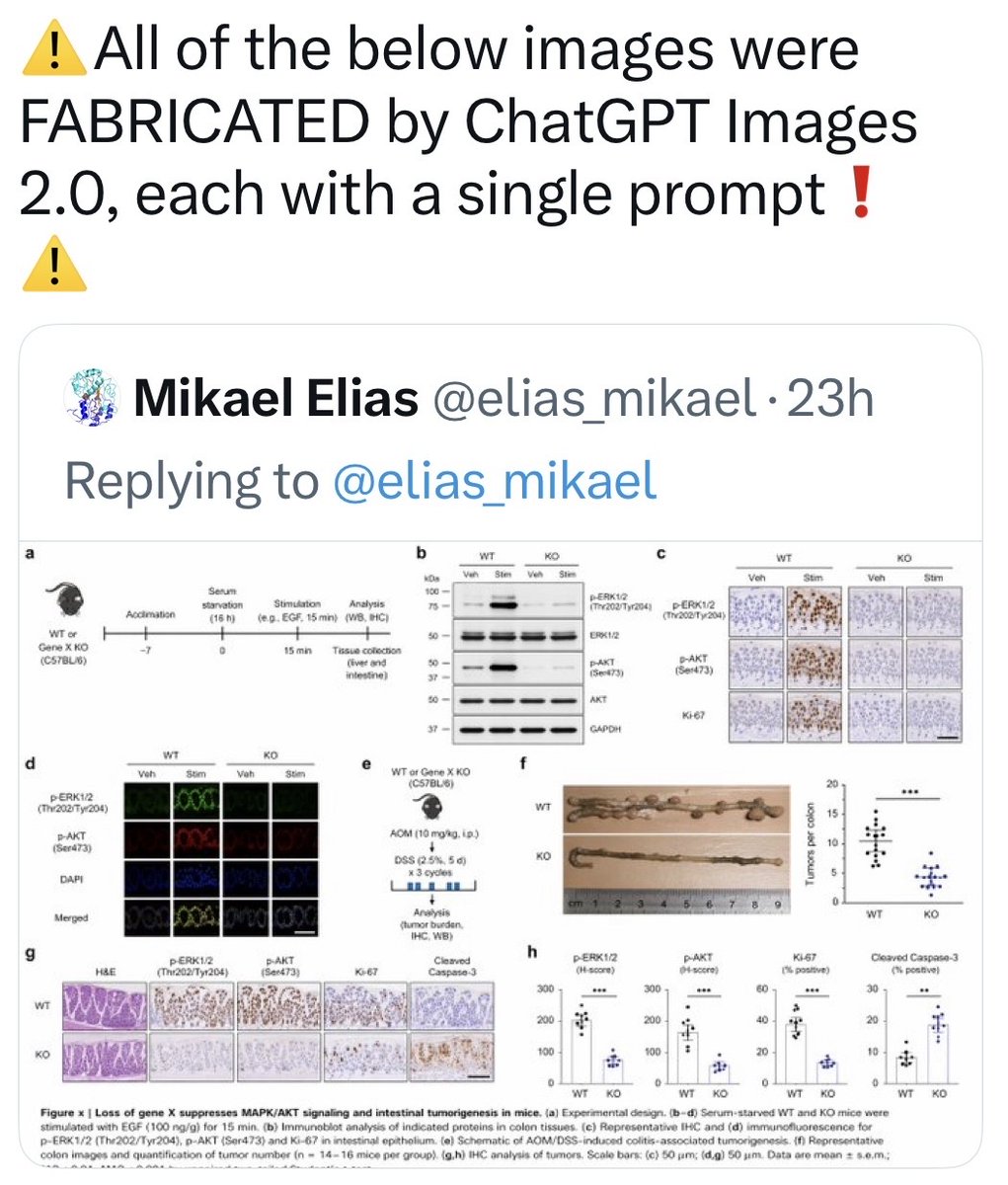
⚠️All of the below images were FABRICATED by ChatGPT Images 2.0, each with a single prompt❗️ ⚠️


🔥@UrolOncol April issue! #TestisCancer RPLND in stage II ECP NSGCT 1⃣ 85% cured by primary RPLND alone 2⃣Oncologically safe and effective when performed at high-volume centers 3⃣Results in less secondary therapy and reduces treatment burden 🔗bit.ly/4cwBEIr