Sabitlenmiş Tweet
Rob Gray🧢
6.7K posts

Rob Gray🧢
@robgraymd
✋ & Microsurgeon. Mayo Clinic, Rush & Brown. “I treat it like it’s my own hand” Opinions my own & this isn’t medical advice
Chicago's North Shore Katılım Nisan 2015
977 Takip Edilen2.3K Takipçiler


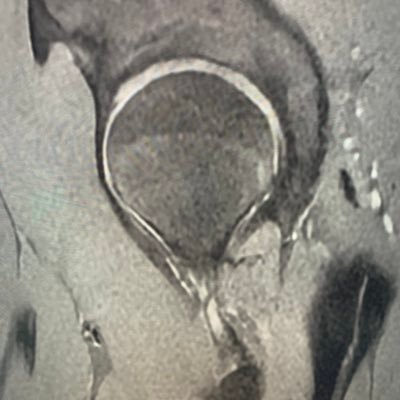
The “broken DISH”
If you know what this refers to, we can be friends
[if you don’t know, we can also be friends]

English
Rob Gray🧢 retweetledi

Here is a clip from our latest episode of CoinFlips & Controversies, “Subacute Elbow Terrible Triad Fracture-Dislocation in 60F.”
Watch Drs. Hoekzema & @robgraymd, discuss “Managing Chronic Elbow Dislocation with Instability, Fracture Fragments, and Nerve Risk."
Click here to learn more and watch their full webinar on Orthobullets: orthobullets.tiny.us/05142026
#orthotwitter
English
Rob Gray🧢 retweetledi

Nobody told you this about success: Rent is due every single day. A lot of people seem to think that after you make it you can coast in the idyllic land of success. This is wrong. Every single day, you have to fight to earn your seat at the table. And that fight gets more intense as you have more success. You have more to lose. More mouths to feed. More people counting on you. More expectations. There's an old saying that I love: Every morning in the savannah, the gazelle wakes up and knows it must outrun the lion or be killed. The lion wakes up and knows it must outrun the gazelle or starve. Whether you're the gazelle or the lion, when you wake up in the morning, you'd better start running. Rent is due daily. Pay it with pride.
English
Rob Gray🧢 retweetledi




@generalorthomd Did I just read that your kids are earning income and could potentially get all of that income tax free and you could write off their income as an expense against the farming revenue and you could put their income into a Roth IRA that has 70+ years to grow???
English

When I’m not doing bone or mountain things, I grow hay. About once a quarter my kids help.

English
Rob Gray🧢 retweetledi
Major life hack: Don't complain, ever. Nobody likes a complainer. They drain the energy of everyone around them. It's exhausting spending time around someone who constantly complains about things outside their control. If it’s within your control, go do something about it. If it’s not, you’re just wasting energy thinking about it. Complaining gives too much power to the thing. Take back that power.
English
@northwoods1980 Seizures are hard to remember. I’m sure this is how he experienced it.
English




Rob Gray🧢 retweetledi

Now I’m going to flip it.
Tricare has the VA pharma contract. @ewarren tried to get a copy of their contract, with pricing to the taxpayer. They won’t provide it.
She has done a good job trying to get to the bottom of their pricing. They refuse.
I’d be willing to bet the President a dollar, they wouldn’t give a copy of the complete tricare contract, with pricing, to him.
The big PBMs, and insurance companies that own them , don’t care what the President thinks and they are not afraid of him or HHS. They are Too Big To Care.
I testified that for many generics, the @costplusdrugs price is less than the tricare, off base co-pay (and that’s before the unknown price the charge taxpayers for the drugs)
When those drugs get on TrumpRx, it will save service members on their medications
Bigger picture, it shows the insanity of our healthcare economics.
Mark Cuban@mcuban
TrumpRx is not a scam. Is it perfect ? No. That would require them to add all @costplusdrugs meds ! They have done a great job on IVF and GLP1s. If it allows a couple to afford to grow their family or to afford the GLP1 they need, it’s a win.
English
I’m not saying it’s technically impossible, I’m saying that unless the machines get logarithmically better at building themselves, you won’t be able to replace human surgeons for the money they pay us.
Noah Kaufman, MD@noahkaufmanmd
If you think surgery won’t be replaced by AI/robotics in the next decade, I think you’re actually nuts. 🤯 instagram.com/reel/DXuxGGRFU…
English
Rob Gray🧢 retweetledi

Learn to lift heavy weights or start saving up for the nursing home.
English

This is one of the most useful productivity unlocks with AI that I've experienced since I first learned about chatGPT.
If you don't know what this is... you're falling behind.
English
@CanesDavid Wow. I have been using ChatGPT, grok, and the occasional Gemini and manus. People keep telling me how great Claude is. Should I add that too/ ditch something else?
English
This is pairing Claude cowork (desktop app) with Obsidian (free) to create essentially an operating system or a second brain which catalogues is everything about you and how you work. When you do this, the output you get is meaningfully better and that’s an understatement.
You’re watching AI construct your personal knowledge base
English
Rob Gray🧢 retweetledi

That some achieve great success, is proof to all that others can achieve it as well.
- Abraham Lincoln
English
Rob Gray🧢 retweetledi

Today AMGA compensation benchmarks went live on Marit. That makes us the only place clinicians can pull three independent comp sources, AMGA, MGMA, and 25,000+ real salaries from clinicians themselves, all in one search and all completely free.
When we launched Marit last year, the problem we set out to solve was the information asymmetry. While employers have access to sophisticated tools and multiple benchmarks to make comp decisions, clinicians had nothing to refer to.
So we built the largest real-time source of clinician-reported comp, by clinicians and for clinicians. Base, total comp, bonuses, call schedule, benefits, satisfaction. Down to the city level, and updating in real-time.
A few months ago we made MGMA free on Marit for verified clinicians, making us the only place where you can get access to free MGMA data.
And today AMGA joins it. Three independent sources, side by side, no paywall.
More transparency drives better matches for both clinicians and employers. Happy to take one more step toward it.
English
@NavalismHQ @naval And if you want to change the world, the best way is to change yourself
English



Rob Gray🧢 retweetledi

I call it Spilled Milk Syndrome.
The people who suffer from it live difficult, stressful lives, no matter how well things may otherwise be going for them.
They freak out when their iPhone screen cracks. Their flight gets delayed an hour, and it makes them crazy.
Their uber driver cancels last minute, and they yell at their screen. Their printer runs out of paper when they’re running late and need that important document - and their heart races like crazy.
Their blood boils when their latte’s too hot. Or their new shoes get stained the first time they wear them. Or the babysitter’s running 10 minutes behind.
Life’s little annoying moments shock them every time. They are the spilled milk moments that fill all of our lives - and they’re routine no matter who you are or even how wealthy you may be.
The people who expect these moments and take them in stride have an incredible gift.
When a business deal falls apart, they try to save it - and they move on to the next when they realize they can’t.
When the baby starts crying again at 3am, they can choose to be frustrated and to feel sorry for themselves because they had a long day and need the sleep - or they can choose to not to let it get them down.
How you handle those countless moments is simply up to you.
They are going to keep happening no matter what - and you can choose to take them in stride, not let them set you back, and to look forward.
Or you can choose to waste much of your life angry and frustrated, “crying over spilled milk.”
It’s perhaps the most important life choice you can make.
English
And if you can make a lot of money, you can get in shape. The worst lie I ever told myself was that I wasn’t a “gym guy.”
Dan Go@CoachDanGo
If you can get in shape you can make a lot of money. The disciplines are almost the same.
English