Sabitlenmiş Tweet

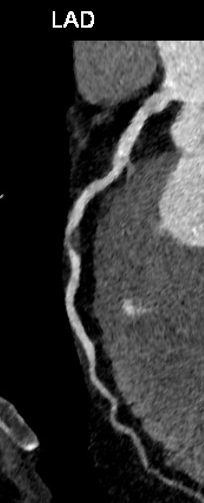
Posted with permission. 57 male screening CTCA after heart concern. Asymptomatic. Rx OMT - ACE-I Statin ASA. CMR - Lifestyle advice given. Any other suggestions? @DrDerekConnolly @DrScottMurray @LondonCardiacCT @NickCurzen @mirvatalasnag @ColinBerryMD @HRahbi @danmckenzie73
English