
Our lead extraction experience @Texas_Heart and @bcmhouston published online in Cardiovascular Drugs and Therapy.
rdcu.be/e86d2
English
Mihail G. Chelu, MD, PhD
1.9K posts

@MihailChelu
Physician-scientist | Professor | Director Research @Texas_Heart and Director of EP @BCMHouston | co-PI with @KennethEllenbo1 of @leftvsleft RCT




📅Mark your Calendar for the Ali Massumi Cardiac Arrhythmia Symposium 2026 📍The Westin Houston Medical Center January 31, 2026 Register here: bit.ly/4pJszAJ @Texas_Heart @BCMHeart @bcmhouston #CardioEd @MihailChelu

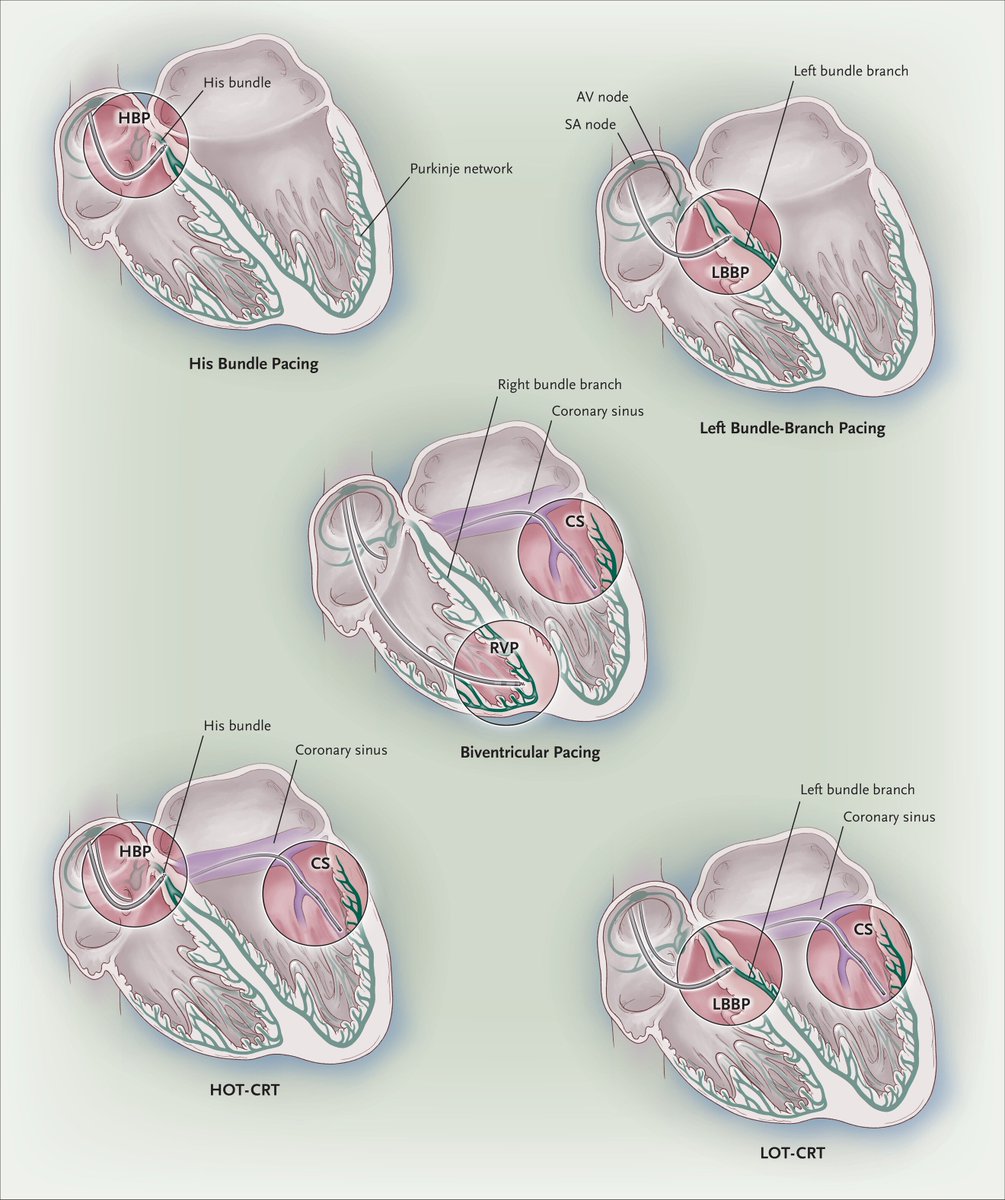
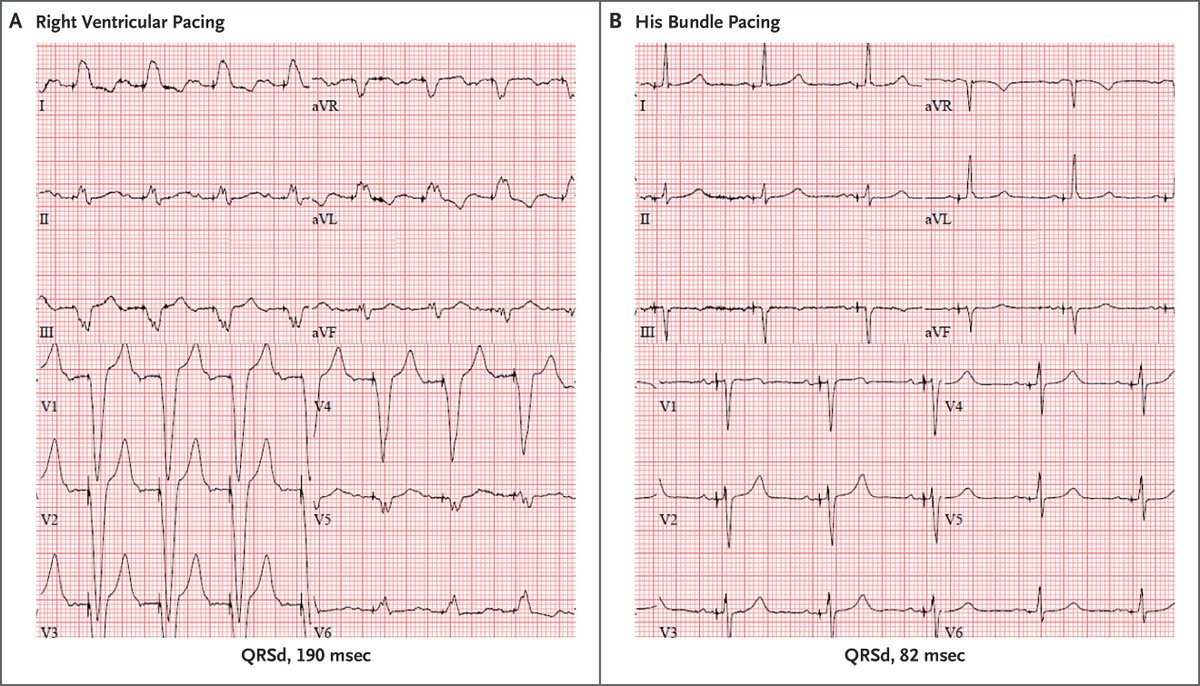

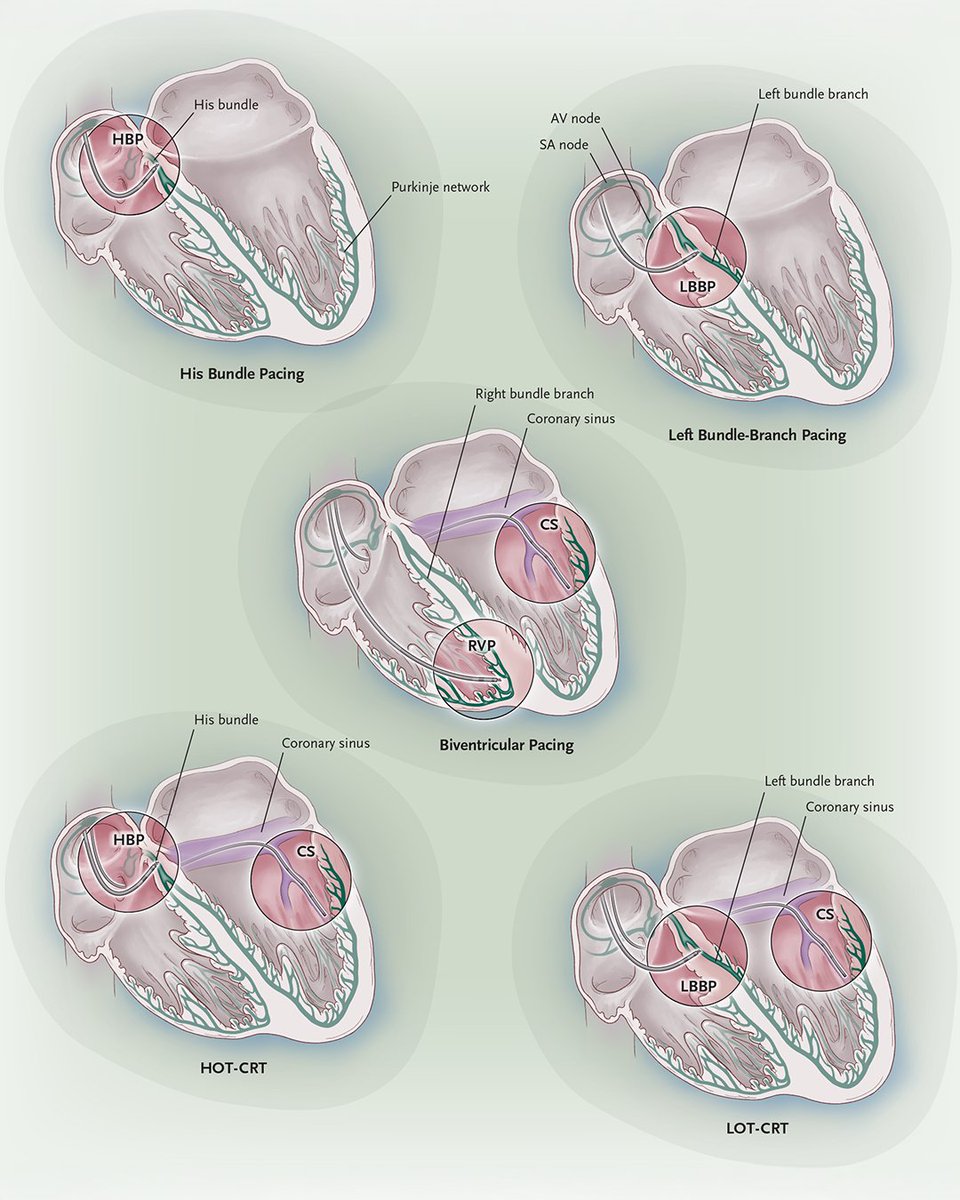
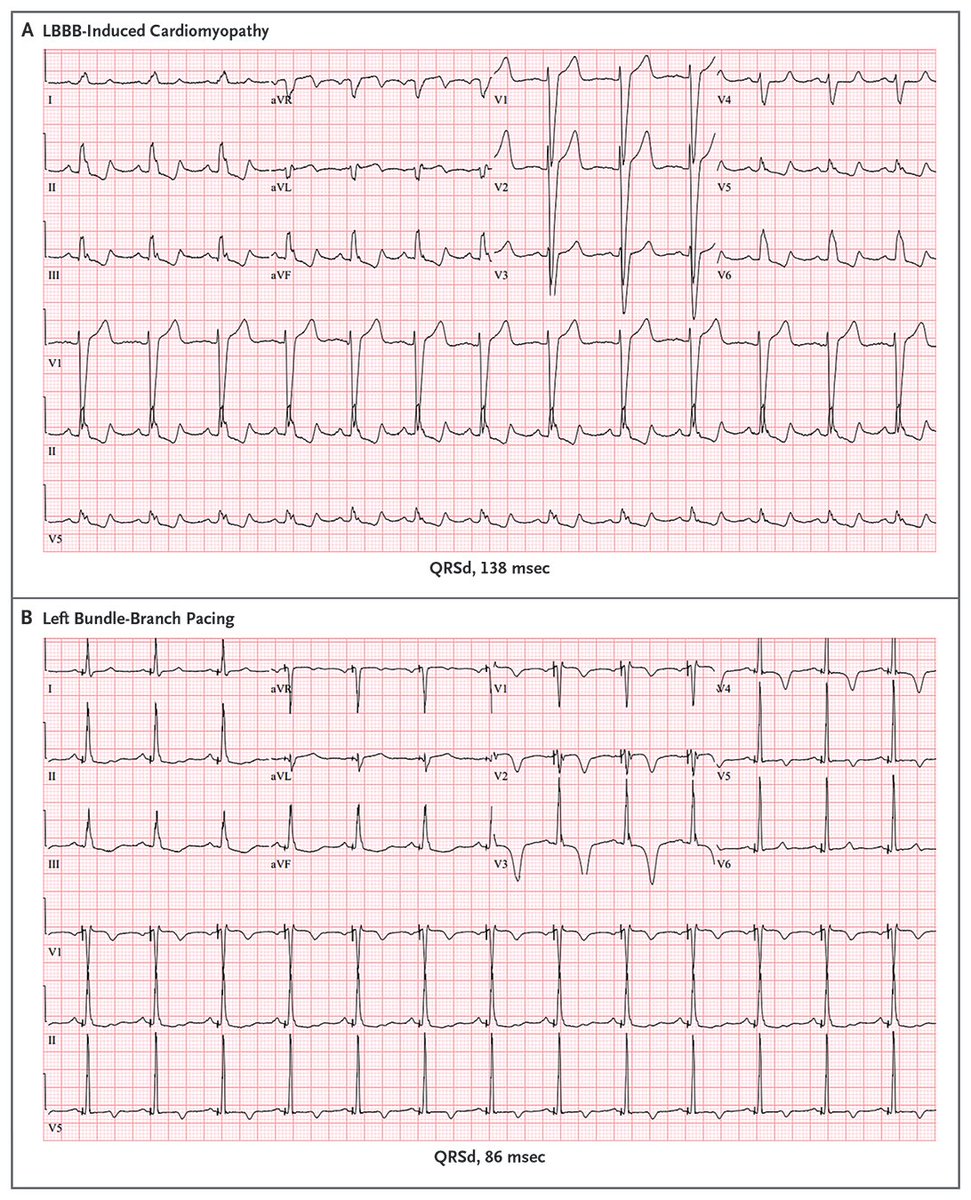
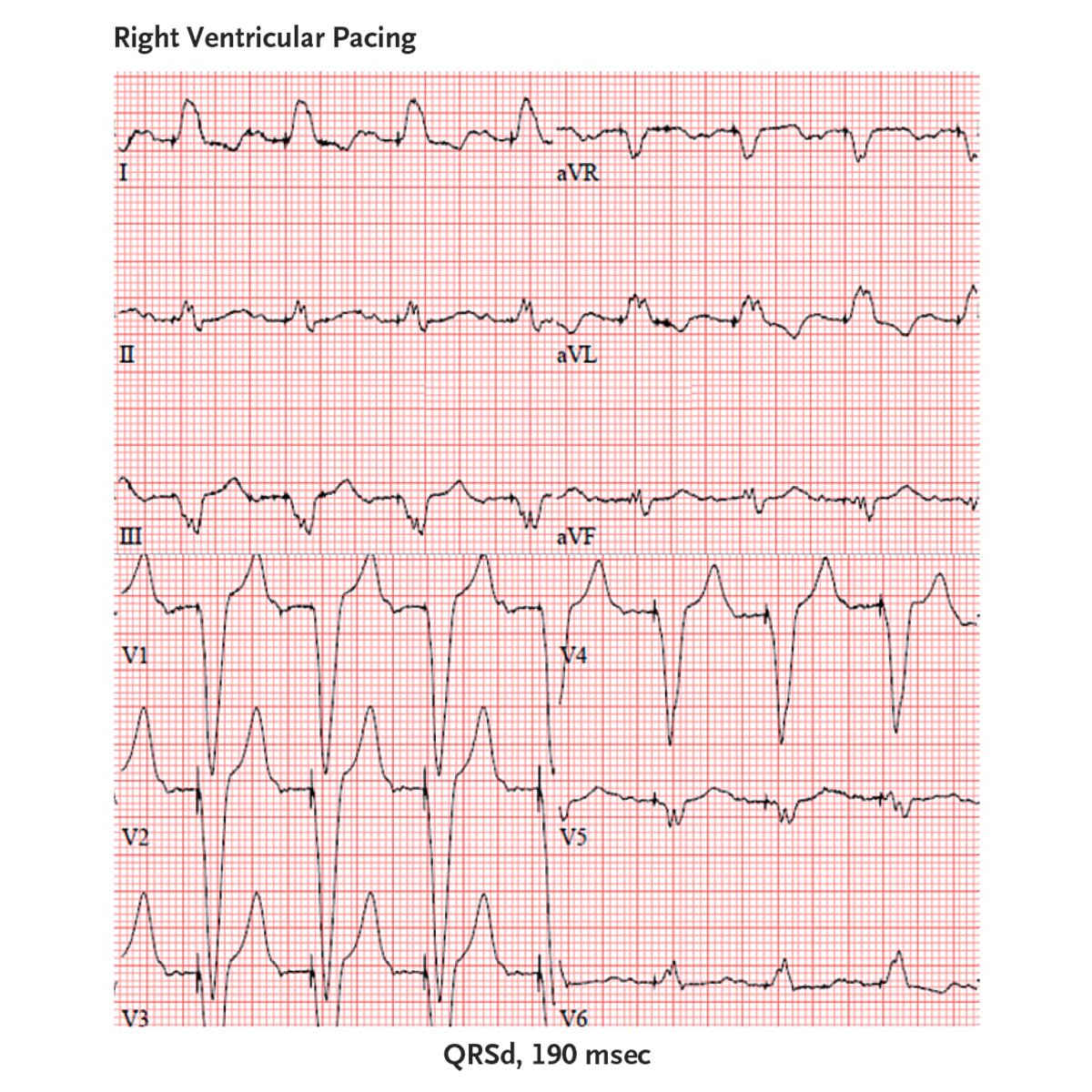
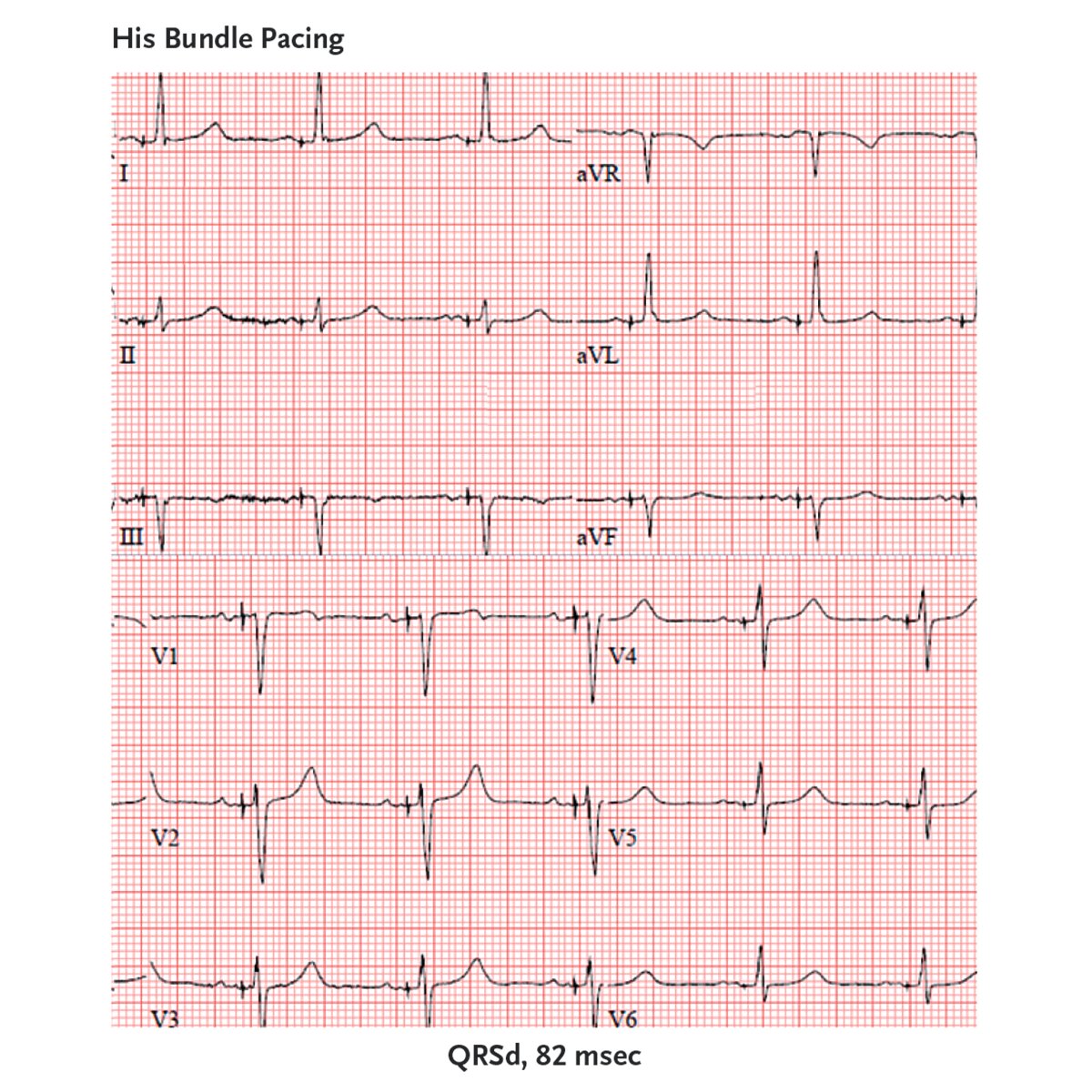
Cardiac physiologic pacing, also known as cardiac resynchronization therapy, is indicated in patients with heart failure, reduced left ventricular ejection fraction (LVEF) of 50% or less, and either a high (or anticipated high) ventricular pacing burden or a wide QRS complex. Traditionally, physiologic pacing has been achieved with biventricular pacing with a right ventricular lead and a coronary sinus branch lead. Randomized trials involving more than 10,000 patients with heart failure have shown clinical, exercise, and quality-of-life benefits associated with biventricular pacing, as well as improved LVEF and reduced mitral regurgitation and ventricular volumes. These benefits are greatest in patients with left bundle-branch block and a QRS duration of 150 msec or longer. Recent studies support targeting the His bundle or left bundle branch as an alternative cardiac physiologic pacing strategy. Ongoing randomized trials are expected to more clearly define the comparative efficacy and safety of conduction system pacing as compared with biventricular pacing. Read the Review Article “Physiologic Pacing in Heart Failure” by @MihailChelu, MD, PhD, Jeanne E. Poole, MD, and Kenneth A. Ellenbogen, MD (@KennethEllenbo1), from the Baylor College of Medicine (@bcmhouston), University of Washington (@UW), and Virginia Commonwealth University School of Medicine: nej.md/4qqjSfI






The TRAVERSE trial shows reduced risk of acute brain lesions with transeptal approach in patients undergoing left ventricular catheter ablation, compared to a retrograde aortic approach. ahajournals.org/doi/full/10.11…


