Carlo Alberto Artusi retweetledi

Adults with the highest levels of physical activity at midlife and late life had 41% and 45% lower risk of all-cause #dementia, compared with those with the lowest levels of physical activity. ja.ma/4i732iN
English
Carlo Alberto Artusi
548 posts

@ArtusiScience
Neurologist - Neuroscience - Parkinson



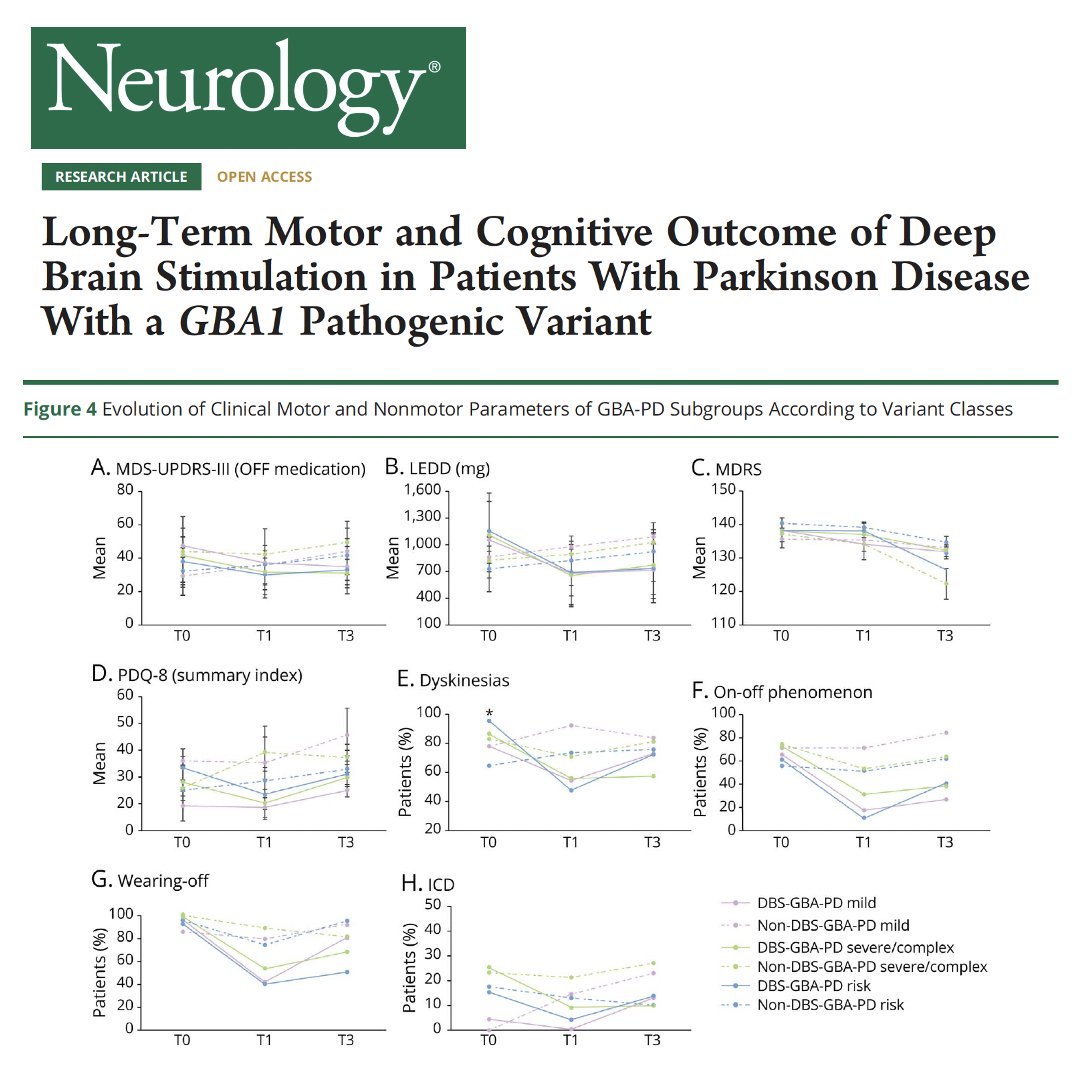





How will DBS go if you have a genetic form of Parkinson's disease? Great new study on the motor and non-motor DBS outcomes using a multi-scale meta-analysis by Asimakidou and colleagues @MDCP_Journal. Key points: - The authors point out we have high-throughput sequencing techniques so why not genetically stratify Parkinson's folks? - They opine this could be added to selection procedures, levodopa challenge testing and may even predict outcome. - They looked at 380 genetic PD cases. - Their conclusion was that genetic PD were as a group 'good candidates.' - Outcomes may differ by mutation. - PRKN benefited most by motor function, daily dose medication and motor complications. - GBA carriers 'appeared' to be 'more prone to cognitive decline after subthalamic nucleus DBS.' - Possible cognitive worsening in SNCA carriers. - Across the board pre-operative levodopa responsiveness and a younger age of onset had better outcomes, which we already knew. My take: Dr. Foote and I are now into our 3rd decade of performing DBS and guess what? We did not always have genetics and most of the time we operated without this information. Over time, we learned that the multidisciplinary evaluation and the careful examination for Parkinson's disease is adequate to make DBS decisions even without genetics. We also learned that folks with GBA mutations can do very well with DBS and that we should be careful not to mix 'general information at a cohort level' with individual level data. Bottom line: If you have a gene underpinning your Parkinson's disease you will likely do well with DBS, however this does not obviate the need for a multi-disciplinary evaluation. So, please take the genetics in DBS candidates with cum grano salis, with a grain of salt, and if you decide to use the information, pair it with other factors such as where a person may be in the progression of their disease. …mentdisorders.onlinelibrary.wiley.com/doi/10.1002/md… #Parkinsons #Genetics #geneticcounseling






How interesting, did you know that increased size of choroid plexus, that unpleasant looking mass of vessels in the cerebral ventricles, is linked to neurodegeneration severity in Parkinson's disease. If you're as interested as I am, read more here 👇 👇 bit.ly/3r8zxqi


In this study, a generative artificial intelligence (AI) model provided the correct diagnosis in its differential in 64% of challenging cases and as its top diagnosis in 39%. ja.ma/3X5M6i9