Ashish Sharma retweetledi
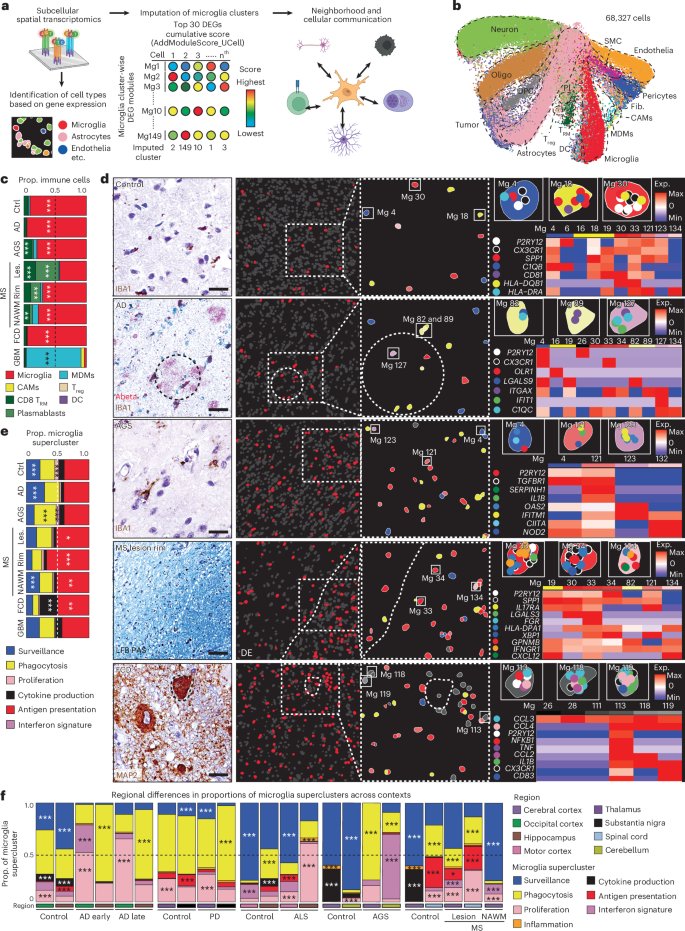
A transcriptomic microglia taxonomy across mouse and human pathologies @NatImmunol
nature.com/articles/s4159… 🇩🇪
Français
Ashish Sharma
309 posts


@asharma313
Postdoc @WashUNeurology with @ErikMusiek studying circadian rhythm and sleep in Alzheimer’s disease








Our glial circadian atlas in AD and aging mice is now out in @NatureNeuro! Congrats to @patwsheehan for incredible work and to our collaborators @johnthefryer, @CarpeRibosomam, @darshan1s, Ron Anafi, and the team. @johnthefryer and I started this in 2019! nature.com/articles/s4159…

I'm excited that @Jjiyeon_lee's 2nd paper from the lab is out in @NatureAging. We found that the circadian gene REV-ERBalpha regulates brain NAD+ by controlling CD38 in astrocytes. REV-ERB KO or pharmacologic inhibition mitigates tau pathology in mice. nature.com/articles/s4358…







The new paper from the Gan lab out today in Immunity shows the Christchurch mutation in the APOE3 gene confers resilience against tau pathology via inhibition of the cGAS-STING-IFN pathway. Congrats to @naguib_sarah , @EiRuTorres, @ChloeLopezLee et al! cell.com/immunity/fullt…
