@ThinkingCC @YubSedhai If suspicion is acute stent thrombosis wouldnt dobutamine in an hypoxic RV just increase RV O2 consumption and increase infarction size? No real right answer IMO. Would rush back to cath.
English
Pablo Cotera
9.7K posts
@pjcotera
Kharon del Mapocho y la Chimba, a contrata. Colchanino. Residente de facho-pobrelandia Ja/ja/ja

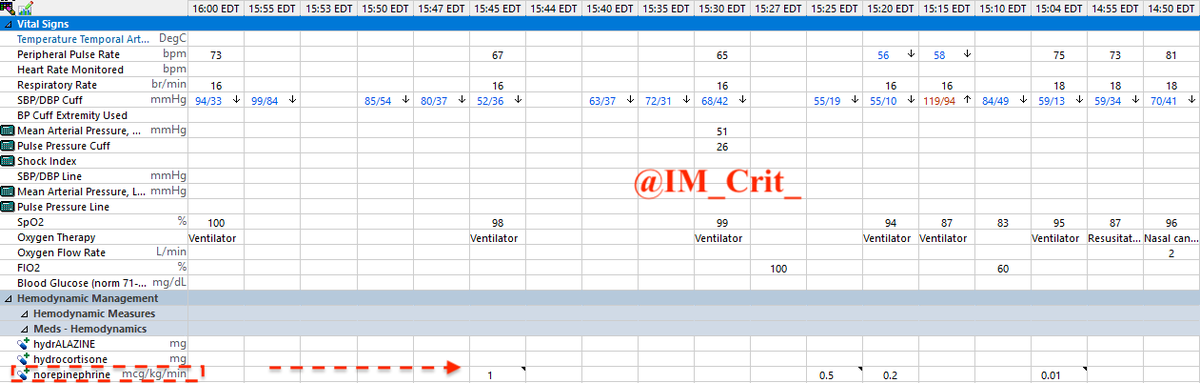
What is the most reasonable immediate next step?





Seed oils: Are they even correlated with bad health? I assembled ALL of the available NHANES data and linked as much as possible of it to the National Death Index and found that... It's not. Seed oils aren't even correlated with problems.

ACVC 2026 | Not all high risk pulmonary embolism is equal. A key message from #ACVC26: 👉 High risk PE is not a single entity, there is major heterogeneity in presentation, physiology, and response to therapy. ⚠️ Guidelines vs real-world complexity According to ESC 2019: • Immediate anticoagulation • Systemic thrombolysis → first-line therapy (Class I, Level B) • Surgical embolectomy → second-line • Catheter-directed therapy (CDT) → third-line ➡️ However, this linear model does not reflect clinical reality 🚨 Limitations of systemic thrombolysis Key concerns highlighted: • Not always fast enough in critical patients • Variable effectiveness on clot burden • Significant bleeding risk • Many patients have contraindications 📊 Important insight: 👉 Up to ~1/3 of PE patients have contraindications to fibrinolysis ➡️ Leading to underuse even in eligible cases 🧠 Not all high-risk PE behaves the same New paradigm (AHA/ACC 2026): High-risk PE spectrum includes: • D1 → transient hypotension • D2 → normotensive shock • E1 → persistent hypotension • E2 → refractory shock / cardiac arrest ➡️ Particularly important: Normotensive shock = high risk despite “normal BP” 🔄 Treatment failure must be anticipated Clinical warning: • Lack of improvement within 24–48h after anticoagulation • No response 2–4h after thrombolysis ➡️ Should trigger escalation ⚙️ Catheter-directed therapies (CDT) Emerging central role: • Can be used early in selected patients • Especially when: Thrombolysis contraindicated Thrombolysis failure Rapid deterioration Algorithm highlights: • Early CDT after indication established • Can follow systemic thrombolysis if insufficient response • Requires PERT-based decision making. 🚀 Mechanical thrombectomy (CAVT) Highlighted as a promising strategy: Advantages: • Rapid clot removal • Immediate hemodynamic improvement • Lower bleeding risk vs systemic lysis Potential benefits of medium-bore devices: • Better distal reach • Lower vascular complications • Faster procedures • Reduced blood loss 🎯 Beyond pulmonary embolism CAVT applications extend to: • STEMI with high thrombus burden • Peripheral arterial embolism • Deep vein thrombosis • Ischemic stroke ➡️ Suggesting a broader paradigm shift in thrombosis management 🎯 Take-home message High-risk PE is not uniform. • Risk stratification must be dynamic • Normotensive shock is critical to recognize • Thrombolysis is not always sufficient or safe • Early escalation and device-based therapies are key 👉 We are moving from a “one-size-fits-all” to a personalized, physiology-driven approach #ACVC26 #PulmonaryEmbolism #InterventionalCardiology #CriticalCare #Thrombectomy #Shock #ESC

El exterminio de pingüinos 🐧 y otras especies de #Chile tendrá nombre y apellido. Sería un documental para la historia oscura de #Chile 🇨🇱